
BLOOD PRESSURE AND ITS MEASUREMENT
Blood pressure (BP) is the pressure that blood flowing in our arteries exerts on the vessel wall. Arteries are blood vessels that carry blood rich in oxygen from the heart to different parts of the body.
This pressure is maximum (systolic BP) when the heart contracts during the heartbeat and ejects the blood into the artery (aorta). The pressure is lowest (diastolic BP) between heartbeats. Therefore, blood pressure is expressed in tmm of mercury (Hg) as a fraction of systolic over diastolic BP (example – 120/80 mmHg).
BP is measured by a machine with an appropriate cuff size and calibration. For any BP measurement, one should be at rest for at least 5 minutes (with no exercise, smoking, or coffee intake 30 minutes prior), and preferably pass urine before a BP measurement. BP is measured while sitting relaxed and comfortably, preferably with a backrest, and feet flat on the ground. The BP instrument and one’s arm are rested on the same table level with the heart. If lying down, the BP machine should be beside at the same level. Sitting BP is usually 5-10 mm more than lying (supine) BP, while standing BP is the lowest. If one has a tendency for dizziness (orthostasis), the difference between sitting and standing BP should be measured.
DEFINING AND STAGING HIGH BP (HYPERTENSION)
Hypertension is globally classified based on BP measurement defined by the International Society of Hypertension, American Heart Association (AHA), and American College of Cardiology (ACC). Hypertension classification and its guidelines are also given by the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). There are differences in these classifications in terms of defining hypertension and the terminology used, as shown below. As per the 2025-26 AHA/ACC BP classification are as follows:
- Normal – systolic <120; diastolic<80 mmHg
- Elevated – systolic 120-129; diastolic <80 mmHg
- Hypertension: 2 stages
- stage 1 – systolic 130-139; diastolic 80-89 mm Hg
- stage 2 – systolic ≥140; diastolic ≥90 mm Hg
BP indicates blood pressure based on an average of ≥2 careful readings obtained on ≥2 occasions – Adults with Systolic and Diastolic BP in 2 categories should be designated to the higher BP category.
The ESC-ESH defines category 1 as non-elevated (BP<120/70), category 2 as elevated (120–139/70–89 mmHg), and category 3 as hypertension (≥140/90 mmHg). Many countries have their own national guidelines and classification based on local lifestyle and risk factors.
It is to be emphasized that a single BP reading is not diagnostic and is not used for decision-making. BP categorization is based on an average of ≥2 carefully obtained BP readings on ≥2 occasions. Adults with systolic and diastolic BP in 2 different categories should be designated to the higher BP category. If the first visit BP reading is high, it should be rechecked (after 1-2 weeks for BP between 160/100 to 179/109 and 2-4 weeks for BP between 130/80 to 159/99).
If the BP reading is 180/110 or higher at any visit, it is treated as an emergency and will need to be immediately managed medically.
Also, the cut-offs mentioned so far are for in-clinic BP measurement. Sometimes, self BP measurement at home (to prevent BP and heart rate rising due to anxiety/nervousness) or continuous BP measurement over 24 hours (ambulatory BP monitoring -ABPM) may be advised. In such cases, the BP cutoffs for hypertension may be even lower.
Orthostatic hypotension (orthostasis) is a rapid drop in blood pressure, typically >20/10 mmHg upon standing, causing dizziness, lightheadedness, or fainting. It occurs when the body cannot quickly adjust to the effect of gravity pulling blood to the legs.
RISK FACTORS
The risk factors described increase the risk of developing hypertension and cardiovascular disease, and their complications. Increasing age and male gender are natural risk factors (an elderly male is more likely to have hypertension as compared to a young female adult). People of South Asian and African races also have a higher risk of developing high BP compared to the white race.
Other risk factors include:
- Being overweight or obese (high BMI)
- Dyslipidemia (increased cholesterol +/- triglycerides in the blood)
- Psychosocial stress
- Sedentary lifestyle or inadequate physical activity
- Smoking
- Drinking too much alcohol
- Psychosocial stress or suppressed anger
- Diabetes
- Kidney disease
- Sleep apnea
- Long-term use of medicines: certain painkillers, decongestant medicines for cold, antidepressants or antipsychotics, oral contraceptives, corticosteroids, and anti-cancer drugs.
- Family history of high BP
- Women post-menopause, or who had hypertension or diabetes in any of their pregnancies.
Salt intake as a risk factor – Salt-sensitive hypertension (SS-HT) is a form of high blood pressure where sodium from salt intake causes a significant increase in blood pressure (5mmHg or more), impacting about 50% of hypertensive individuals and causing higher cardiovascular risk. Salt-resistant (SR-HT) hypertensive individuals, by contrast, maintain stable blood pressure despite changes in salt intake due to efficient kidney sodium excretion. SS-HT has a higher prevalence in African Americans, the elderly, women, and individuals with diabetes or chronic kidney disease (CKD).
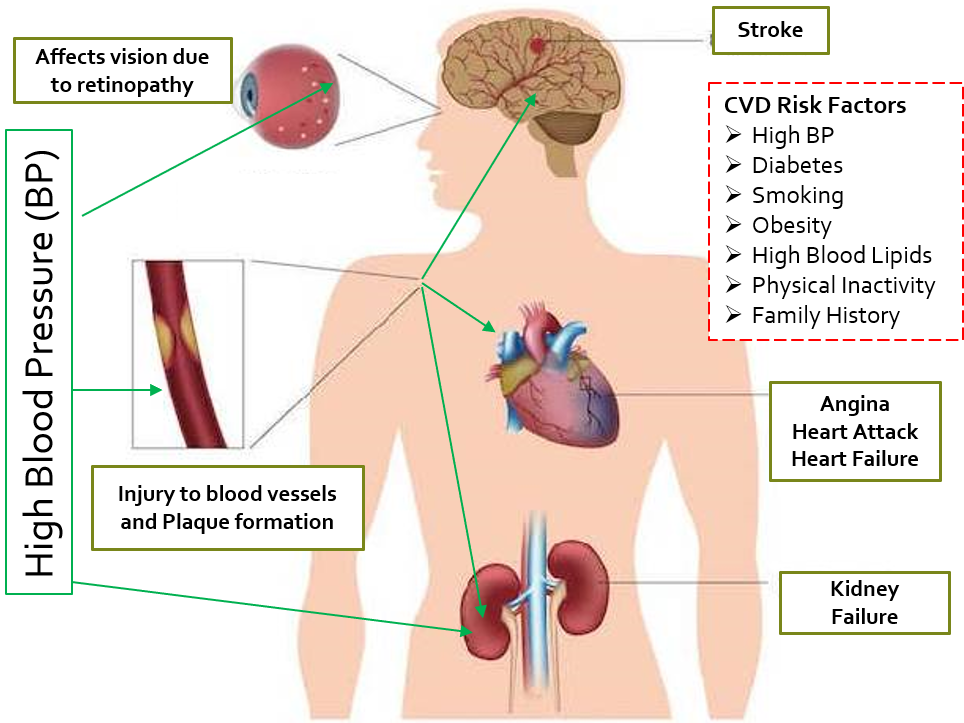
CONSEQUENCES AND COMPLICATIONS OF HYPERTENSION
High blood pressure, especially when not adequately or well controlled, can lead to consequent complications.
Cardiovascular disease (CVD) refers to a group of conditions occurring due to blockage of blood vessels, more specifically arteries, and their resulting impact on the heart and other organs.
Blood flowing at higher pressure has more chances of causing micro-injuries to the artery wall. This gives rise to increased formation of ‘plaques’ and clots, which cause narrowing or obstruction of arteries, leading to CVD. This can result in a reduction (partial obstruction) or loss (complete obstruction) of blood supply to vital organs. The above risk factors mentioned for hypertension are also risk factors for developing CVD. High blood pressure increases the risk of CVD, and vice versa, while both CVD and hypertension may present simultaneously.
CVD can result in angina, heart attack (myocardial infarction), stroke, and peripheral arterial disease (PAD). Angina and myocardial infarction (MI) are caused by partial and complete blood flow obstruction to the heart, respectively, which causes heart pain due to oxygen deprivation to the heart muscles. Since the heart has to pump blood against higher pressure and resistance, its contracting effort increases, which can slowly lead to its reduced efficiency and inability to cope, causing heart failure.
Obstruction/reduction in blood flow to the brain leads to stroke (also called cerebrovascular accident, CVA). High BP can also affect blood flow to our limbs (peripheral arterial disease), which can cause intense pain on walking.
Hypertension can cause ongoing damage to the kidneys and eventual kidney failure.
Other complications, like rupture or blockage of the fragile, narrow vessels of the retina of the eye (hypertensive retinopathy), can affect vision. Hypertension can cause a reduction in blood flow and damage to many other organs, such as bones, reproductive organs, and others, hampering their functioning.
High/uncontrolled BP and CVD are risk factors for complications of COVID and other infections in those who get infected and have these comorbidities.
Complications of high BP are shown below.
HEALTH SOLUTIONS
Overall more the number of coexisting risk factors present in an individual, the greater the risk of developing complications of high BP. Sometimes a 10-year risk of CVD is calculated, and if it is > 10%, BP-lowering medicines are started immediately along with lifestyle-diet measures.
Setting Target BP.
The new default systolic BP target as per both guidelines is 120–129 mmHg. However, the ACC-AHA further suggests a target <120 mmHg when feasible, emphasizing the new “PREVENT” risk calculator, a more advanced risk estimation tool for overall cardiovascular risk, independent of race. It incorporates the risk of heart failure, heart attack, and stroke, and takes into account kidney function, glycated hemoglobin (HbA1C), and urine albumin/creatinine ratio (UACR), covering a wider age range (30-79 years) to provide both 10-year and 30-year risk estimates supporting long-term prevention.
The ESC-ESH advises relaxed BP targets for adults aged ≥85, those with significant frailty, or symptomatic orthostasis. BP in categories of 120–139/70–89 is a major focus for preventing progression, with drug treatment based on cardiovascular risk. Screening for hypertension every 3 years for those <40, and annually for those ≥40 is recommended. Lower target blood pressure recommendations aim to create greater health consciousness of lifestyle and diet, help in early intervention to prevent complications, and maintain a higher level of community health.
So, <130/80 can be considered the new BP target globally from a cardiologist’s perspective. However, many general physicians today would still rather go with the <140/90 target BP, sometimes further relaxed to <150/90 in patients >65 years of age. Therefore, individual factors play a huge role in BP management.
Planning Treatment
People in the stage of elevated BP are managed with lifestyle and diet modifications. These measures can reduce systolic BP by 4-10mmHg, usually in the range of around 5mmHg over a few months.
People in elevated stage 1 hypertension who have coexisting cardiovascular risk factors (or a 10 year CVD risk >10%) will require a BP-lowering medicine in addition to lifestyle-diet measures, as compared to people without additional/coexisting risk factors who can be initially managed with lifestyle-diet measures alone.
All people in stage 2 hypertension should be managed with a combination of BP-lowering drugs and lifestyle-diet modifications.
The target BP of all patients in stage 1 and 2 hypertension is <130/80. However, as mentioned, there may be variability among physicians and cardiologists in setting the target BP in different patients.
For identifying salt-sensitive (SS-HT) patients, the gold standard way is to make patients follow a high-salt diet (e.g., 12g salt/day) for 1–2 weeks, followed by a low-salt diet (e.g., <1g salt/day) for 1–2 weeks, with BP monitored throughout. However, this is usually impractical; therefore, a surrogate way is to do an ambulatory BP and heart rate (HR) monitoring for 24 hours, in which a 24-hour mean HR >70 bpm, paired with a non-dipping pattern (BP fails to decrease by 10% or more during sleep), is considered to indicate SS-HT
Lifestyle and Diet measures for reducing BP and CVD risk
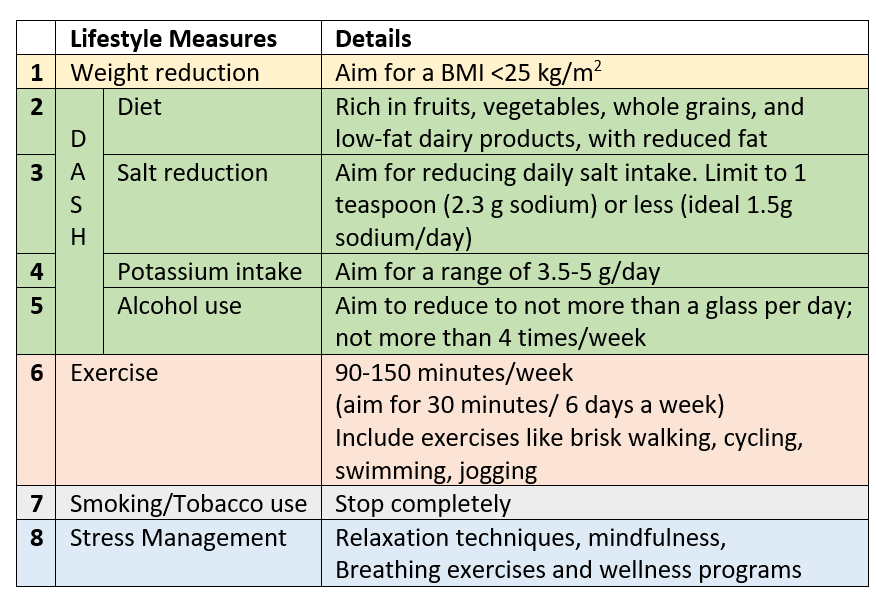
Lifestyle-diet measures for blood sugar and lipids (cholesterol and triglycerides) will be advised if these 2 risk factors coexist with hypertension.
DASH– Dietary Approaches to Stop Hypertension is aimed at lowering BP, reducing the risk of cardiovascular sequelae, and also helping in BMI and weight reduction. It is beneficial for both SS-HT and SR-HT, as well as for obesity, diabetes, and controlling cholesterol/triglycerides. The diet works by balancing nutritional intake, increasing fiber, and maximizing intake of potassium, calcium, and magnesium, which help relax blood vessels and lower pressure.
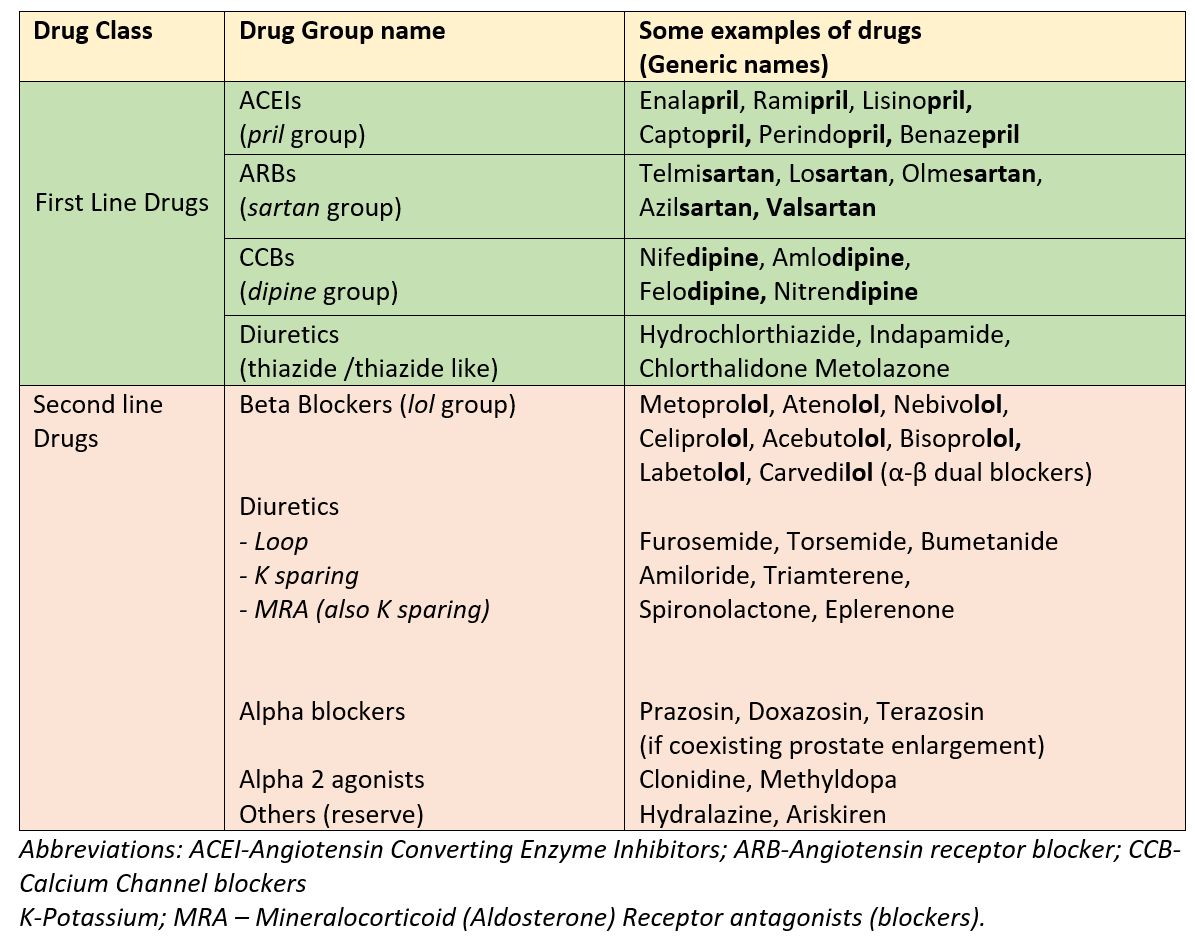
Overview of BP-lowering Medicines
BP-lowering medicines are given singly or in combinations (separately or combined in a single pill). Usually, one medicine is added for every 10mm systolic BP above the target. Sometimes two medicines at lower doses may be preferred to one medicine at a higher dose, to improve response and reduce side effects.
There are 4 classes of BP-lowering medicines that are considered first-line. One of these or a combination of these is used to bring and maintain the BP at target values. The second-line drugs are used when the combination of 3 first-line agents of different classes does not manage to control high BP or in certain special situations or patients with associated cardiac, kidney, or other conditions.
Important points to remember
- All medicines should be taken only by prescription and recommendation of a qualified medical practitioner in the dose, schedule, and time of day prescribed, along with incorporating all the lifestyle and diet measures suggested.
- Separate medicines will also be needed for coexisting risk factors (like diabetes and high lipids) if present.
- Irregularity in taking these pills can lead to uncontrolled BP.
- There are certain situations where some classes of drugs may not be appropriate or suitable, while some may cause side effects in certain patients, so one should never start or change any drug without consulting a qualified physician.
- The blood pressure and parameters for other risk factors, when present, should be measured and monitored periodically under the guidance of the treating physician.
- Usually suggested follow-up visit is at 3 months after starting on lifestyle-diet measures, and at 1 month after starting a BP-lowering medicine.
Some scientific terms
Essential (or Primary) hypertension is high blood pressure that doesn’t have a known cause.
Secondary Hypertension is high BP caused by another medical condition, like diseases of the heart, kidney, arteries, or hormones
Resistant Hypertension is the term used when the target blood pressure below the cut-off cannot be achieved even with lifestyle measures and concurrent use of three BP-lowering medicines (of the 1st line classes, with one of the medicines being a thiazide group diuretic), after ensuring full compliance and regularity of treatment.
‘Uncontrolled Hypertension’ includes resistant hypertension as well as those patients not fully compliant or regular with medicines and/or incorporation of lifestyle measures.
The reserve or 2nd line medicines are then added in resistant hypertension to achieve the target BP. Sometimes, certain procedures (called renal denervation by radiofrequency or ultrasound) may also be used to manage resistant cases.
Preeclampsia is high blood pressure during pregnancy. It can have serious consequences for the mother and fetus, and so needs timely addressal. The first-line drugs below, like ACEI and ARBs, cannot be given in pregnancy due to adverse effects on the fetus. Therefore, preeclampsia is managed by drugs like labetalol, methyldopa, and nifedipine.
References:
2025-26 AHA/ACC Hypertension guidelines
2024 ESC-ESC Hypertension guidelines
Also read-
Cardiovascular Disease (CVD) – Understanding Atherosclerosis and Coronary Artery Disease
For any query, additional information or to discuss any case, write to info@drvarsha.com and be assured of a response soon