
Everyone has suffered from itching at some time or another. Itching is an unpleasant, irritating feeling or sensation on the skin that urges one to scratch. For some, itching is a chronic problem and can be a cause of great distress, especially at night, compromising sleep and quality of life.
TYPES OF ITCHING
Itching (medically called pruritus; plural-pruritis) can be acute (sudden onset – lasting for a short duration of < 6 weeks) or chronic (has been present on and off, or continuously for > 6 weeks).
Itching can be localized (in particular parts of the body) or generalized (all over the body). For localized itching, a skin problem (dermatological disorder or disease) is usually the cause; however, in generalized itching, one may need to investigate for non-skin causes (due to diseases in other organs – systemic causes).
IS THE ITCHING DUE TO A SKIN PROBLEM OR NOT
DRY SKIN
Dry skin is the most common cause of generalized itching. Sometimes the skin hardly looks dry, but when you scratch across it, to your surprise, a white line will appear, indicating underlying dryness! Dry skin can occur in all age-groups, but it increases with age and is a very common problem in the elderly population. Dry skin is not considered a skin disease per se, but can cause a distressing amount of chronic itching and disturbance of sleep.

SKIN INFLAMMATION
Localized itching in particular parts of the body is usually due to skin disease or irritation, and may have some obvious signs on the skin, like a rash. A rash is a change in skin color and texture where the involved part looks red and inflamed, with a patchy or raised appearance, sometimes with blisters, cracks, scales, or swelling. A rash may or may not be painful, but it is commonly itchy.
Skin diseases causing rashes and itching are tabulated below.
Inflammatory skin conditions like eczema, atopic dermatitis, and urticaria (hives) are considered to be allergic, while contact dermatitis is due to irritant substances
Photodermatoses are skin conditions producing skin inflammation (itchy, red rashes, and eruptions) that are caused by an abnormal reaction of the skin to sunlight (usually ultraviolet UV component, but sometimes visible light also). This could be:
- photodermatitis, also called sun poisoning or photoallergy, is a skin reaction to an allergen that is activated by light
- phototoxicity, also called photo-irritation, is a chemically induced skin irritation by light.
- phytophotodermatitis, a condition causing skin inflammation and rash resulting from contact with light-sensitizing botanical (plant-derived –phyto) substances, called furanocoumarins, that contain particles called psoralens that are sensitive and activated by UV light.
Other conditions like psoriasis, lichen planus, and pemphigus/pemphigoid may have an autoimmune etiology (error in the body’s immune recognition and response).
Sometimes, skin scars from wounds, burns, or surgery can also be itchy.
SKIN INFECTION
Skin infections that cause itching are often contagious, like fungal infections, scabies, lice, and viral exanthems (chickenpox, herpes zoster, etc.), while non-infective conditions, like eczema, psoriasis, hives (urticaria), and lichen planus, are not contagious.
Demodex mites are common inhabitants on human skin and its pores and hair follicles, and usually don’t cause any harm. But these mites can multiply in conditions of poor hygiene or low immunity and cause skin irritation and rash (demodicosis). The rash is more common on the face and can, in appearance, mimic acne, but demodex rash is often rough and scaly (sometimes with pustules), associated with itchiness, burning, and skin sensitivity. Eye irritation and itchiness, loss of lashes, and thickened or scaly eyelids may also be seen. Diagnosis is confirmed by skin microscopy, scraping, and biopsy.
RASH AND ITCH-SCRATCH CYCLE
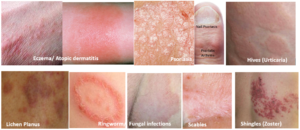
Usually, skin diseases present with a rash before, along with, or just after the itching starts. Most skin diseases have a characteristic pattern and appearance of the rash, which can clinch the diagnosis for a doctor.
However, even if itching is not due to a skin disease, repeated, prolonged, and forceful scratching of the skin induces a lot of trauma, which can lead to a rash developing over a period of time, making it look like a primary skin disease by the time you visit a doctor! So, knowing the timing of the development of the rash and when the itching began is very important.
Scratching itself causes skin irritation, leading to more itching (called the itch-scratch cycle). Severe itching and inflammation also increase the production of melanin (skin color pigment), causing the affected part to darken (post-inflammatory hyperpigmentation -PIH).
SYSTEMIC CONDITIONS
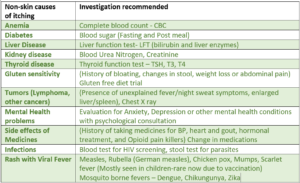
Apart from dry skin, generalized itching may not be due to a skin-related cause and can be a symptom of other organ diseases (systemic causes). These conditions include diabetes, liver, kidney, or thyroid disease, iron deficiency anemia, and mental health causes like anxiety and depression.
Some medicines can also have itching as a side effect, like those for BP, heart disease, gout, hormonal treatment, and pain (opioid pain killers).
During pregnancy and around the time of menstruation, hormonal changes occur, which can, in some women, be a cause of generalized itching.
Itching during menopause is a common symptom driven by declining estrogen levels causing a reduction in the skin’s natural oils and hydration, leading to dry skin, increased sensitivity, and crawling or tingling sensations causing itching throughout the body.
Parasites can sometimes trigger the body’s immune system to release itch mediators like histamines, causing a generalized itch (hookworm “ground itch” or cutaneous larva migrans, filarial worms, onchocerciasis (river blindness), schistosomiasis (swimmer’s itch), and strongyloidiasis roundworm (known as larva currens itch). Such parasites are treated with oral anthelmintic medications such as albendazole, mebendazole, or pyrantel pamoate.
Nerve compressions can sometimes be a cause of itching. Pinching of spinal nerves (typically at the T2–T6 levels) causes a chronic, localized patch of intense itching on the upper back, usually just to one side of the spine. Similarly, nerve impingement in the cervical spine (C3–C6) leads to itching in the forearms and shoulders.
Nerve-related itching, medically known as neuropathic itch, occurs when there is misfiring of nerves that send false signals to the brain. It often presents as a deep, urging, or tingling itching sensation with no visible skin rash, and is unresponsive to standard treatment like moisturizers, antihistamines, or steroid creams. Though some known causes are peripheral neuropathy caused by diabetes, multiple sclerosis (MS), or vitamin B deficiencies, very often no specific cause is found.
Tumors of the liver, bile duct, or pancreas can block bile flow and build up bile salts, resulting in severe itching (often worst on the palms and soles), often with jaundice (yellowing of skin/eyes).
Paraneoplastic syndromes
These can cause severe generalized itching (paraneoplastic pruritus). This is a generalized reaction where a cancer releases inflammatory mediators (like cytokines and bradykinin) into the body, causing itching without a rash. It is most frequently associated with tumors like Hodgkin lymphoma, polycythemia vera (bone marrow cancer), leukemia, and some other tumors.
The itching occurs across the entire body (often worst at night) but on completely normal-looking skin. It frequently causes secondary skin damage from scratching. Paraneoplastic pruritus may also present alongside other systemic symptoms, such as unexplained weight loss, night sweats, or neurological changes.
The itch is notoriously resistant to standard treatment with antihistamines and topical creams, but resolves entirely once the underlying tumor is successfully treated, and can return if the cancer relapses.
WHY IS ITCHING MORE PRONOUNCED AT NIGHT?
Irritation to the nerve endings in the skin is picked up by receptors and relayed as an itch sensation to the spinal cord and brain, which thereafter sends back signals that cause the urge to scratch. The commonest and most well-studied itch mediator is ‘histamine,‘ but other mediators like bradykinin and cytokines are also commonly involved.
Many conditions (both skin and non-skin related), including dry skin, are associated with the itching being significantly more at night. There are many reasons for this:
- There is an increase in skin temperature and more water loss from the skin during the late evening and night, thereby increasing skin dryness.
- The levels of our body’s steroid hormones (which reduce itch and inflammation) are lower at night.
- There may be more release of certain substances in the evening/night, like beta-endorphins (known to lower pain perception but increase itch sensation), and other mediators of itch and inflammation (histamine and cytokines).
- There are fewer distractions at night, cumulated mental stress of the day, sometimes with anxiety or depression, all of which increase itch perception.
Night-time (nocturnal) itching impacts sleep and the next day’s performance and can reduce efficiency in day-to-day life.
HEALTH SOLUTIONS
The specific disease (skin-related or systemic condition) is medically treated accordingly once diagnosed. The following therapies are generally used in treating itchy skin, inflammatory conditions, and rash.
MOISTURIZERS AND SOOTHING AGENTS
Lotions/creams and oils are the first line of management along with lifestyle modification, especially when dry skin is present. Many lotions/creams have natural substances with moisturizing, soothing, and anti-inflammatory/anti-itch properties, which are not only beneficial for relieving symptoms but also suitable for long-term usage due to the absence of any significant side effects. Some of these substances include coconut oil, colloidal oatmeal, aloe vera, tea tree oil, turmeric, honey, shea/cocoa butter, wheat germ oil, and cetearyl alcohol.
Applying such moisturizing lotions/creams, especially at night, bathing in lukewarm water, along with using non-alkaline soaps or bathing oils, are effective solutions.
Calamine is a soothing agent commonly used to relieve acute itching caused by exposure to irritants.
MEDICINES
Antihistamines are a class of oral drugs that are most commonly prescribed to provide symptomatic relief from itching and allergy, and also help improve sleep.
Counterirritants are agents that produce a superficial irritation in one part to relieve irritation/itching in another part. This happens by stimulation of temperature receptors in the skin, which produce a sensation of heat or cold. Examples are creams/lotions containing menthol, methyl salicylate, camphor, thymol, etc. Capsaicin is an effective counter-irritant, especially for neuropathic itch.
Corticosteroids are immunomodulatory medicines that act by suppressing inflammatory mediators of our immune system and are therefore effective in relieving moderate-severe skin inflammation as well as itching. Corticosteroids are commonly part of creams and ointments given for itching and are the cornerstone of managing skin inflammations like eczema and psoriasis. Corticosteroids can range in potency from low (hydrocortisone), medium (triamcinolone, mometasone, beclomethasone), and high (clobetasol, halobetasol). In severe cases, they may be given orally (prednisone, methylprednisolone, dexamethasone) for a limited period.
Other immunomodulatory medicines available are calcineurin inhibitors tacrolimus/pimecrolimus (used in atopic dermatitis), and the vitamin D analog calcipotriol (in combination with a corticosteroid for psoriasis), available as ointments. Methotrexate, cyclosporine, azathioprine, etc., are oral immunomodulators that may be prescribed in some severe cases of psoriasis.
Acitretin is an oral retinoid used in psoriasis that acts by decreasing the scale formation due to the abnormal growth, multiplication, and thickening of skin cells.
Note: Corticosteroids and immunomodulatory medicines should never be used without a doctor’s prescription as their dosing and usage need medical supervision to avert and minimize adverse effects. Acitretin should be used only after pregnancy has been completely excluded, and contraception started.
Biologicals (monoclonal antibodies- MAbs) act by targeting specific components of the immune system that are causing the inflammatory or allergic reaction. These are reserved for severe and unresponsive cases like omalizumab (urticaria), dupilumab, lebrikizumab (atopic dermatitis), and infliximab, adalimumab, and secukinumab (psoriasis).
Anti-infective agents are needed for skin infections, and there are specific drugs for bacterial or fungal skin infections, herpes, scabies, or lice, acting against the causative organisms. It is important not to cause skin damage and secondary infection due to the trauma of recurrent and forceful scratching.
Light therapy in some skin conditions, may be an option that the dermatologist may offer.
Psychological intervention and medication in the form of behavioral modification therapy and antidepressant or antianxiety medicines can also help under appropriate medical monitoring, in select cases of generalized itching.
Gabapentinoids (like gabapentin and pregabalin) are effective, off-label oral medications used to treat chronic, treatment-resistant itching (pruritus), particularly neuropathic or nerve-related itch. They work by blocking overactive nerve signals in the spinal cord, interrupting the vicious itch-scratch cycle.
Hormone Replacement Therapy (HRT) or estrogen creams can address the root hormonal cause in menopause, if conventional therapies do not relieve skin dryness and itching.
Also read-
Skin Infections – Types, Predisposing Factors and Health Measures
Understanding Viral Exanthems – Viral Diseases with Rash and Eruptions
For any query, additional information or to discuss any case, write to info@drvarsha.com, and be assured of a response soon.
References:
Diagnosis and management of chronic pruritus: An expert consensus review
Pruritus: Etiology and patient evaluation
A Diagnostic Approach to Pruritis