
First aid basics are very useful to manage many household and common injuries. It is important to know the do’s and don’ts and also the alert signs for seeking timely medical intervention.
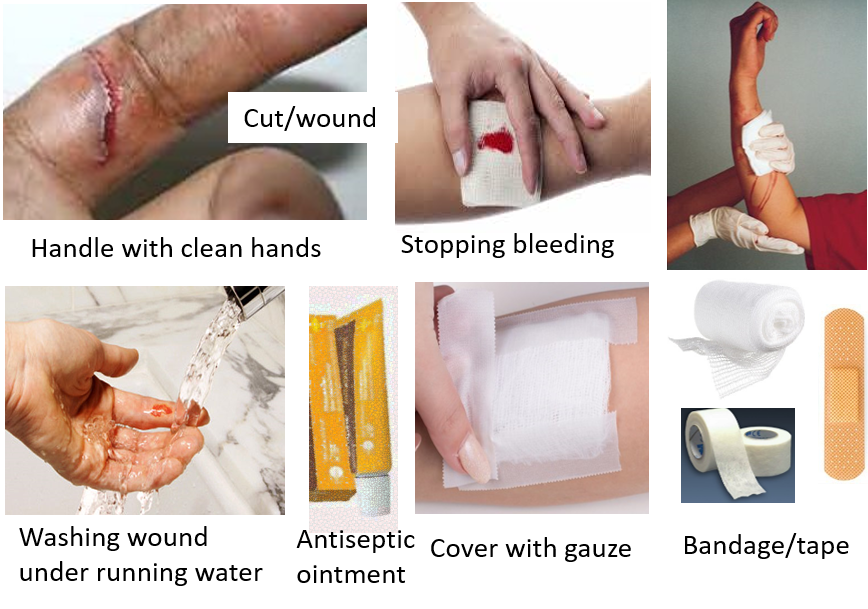
CUTS, SCRAPES AND WOUNDS
- Always wash your hands well before handling wounds and giving first aid
- Gently press the cut/wound with gauze till bleeding stops. The affected part can be raised to stop bleeding faster
- Wash the cut or wound under running water to clean and remove debris. Do not apply soap or cleansing agent on/inside the wound. Cleaning under tap water is easier and more effective than cleaning with antiseptic solutions.
- Applying antiseptic ointment is not required in most cases as this can actually delay healing. Antibiotic/antiseptic ointments are to be used under medical advice if the wound looks infected.
- Cover with sterile dry gauze and adhesive bandage/tape. Do not apply any adhesive tape or bandage directly on wound
- Do not breathe or blow on the cut/wound
- Do not touch the wound edges or interior of the wound with hands
- Do not use cotton for cleaning or covering wounds as they can stick, leave behind strands/threads, and delay healing.
- Do not try to peel of wound scabs.
- Have a first aid kit handy with multiple gauze pieces, bandages, adhesive tapes, antiseptic and gloves.
Visit a doctor if –
- The wound looks deep or gaping with the edges of the wound far apart, as it may require stitches (sutures).
- There is continuing bleeding or oozing even after pressure for 10 minutes, bleeding is occurring through the bandage, or if there is spurting of blood.
- Foreign objects are present in wound despite cleaning under running water.
- Signs of infection are there like swelling, continuing pain or throbbing, oozing of pus, or fever.
- Wounds are on any part of the face, or on/near genitals.
- No tetanus shot has been taken for last 5 years
BURNS
Minor household burns and scalds due to stove fires, hot pans/appliances, boiling water, etc. can be managed at home with effective first aid.
- Put part under cool running water for 10-15 min. Do not use cold water or apply ice.
- Remove jewelry, straps and loose clothing in the vicinity. Do not forcefully pull of anything sticking to burn area.
- Can apply antiseptic ointment on burn area after it is cooled.
- Cover loosely with sterile gauze and bandage.
- Do not apply butter, oils, toothpaste or lotions/creams.
- Do not apply cotton on the burnt area.
- Do not puncture blisters or pull off peeling skin.

Types of Burns
First-degree – These burns involve only superficial layers of the skin. It is mild and presents with redness, pain and swelling followed after 2-3 days by skin peeling. These usually heal in a week without long-term skin changes or scarring.
Second-degree – These burns involve the deeper skin layers but are partial thickness. They present with redness, pain, swelling and blisters. They heal in 2-4 weeks, with some long-term skin changes and scarring. Extensive second-degree burns should be treated under medical care.
Third-degree – These are full-thickness burns. There is usually visible charring and extensive damage to the skin and deeper layers of fat and muscles. Damage to nerves may also occur causing numbness instead of pain. These need immediate medical intervention and treatment with antibiotics. If extensive, hospitalization may be needed to infuse fluids and avoid/manage a drop in blood pressure or shock. Healing may take several weeks to months often with prominent scarring. Skin-grafting is often required.
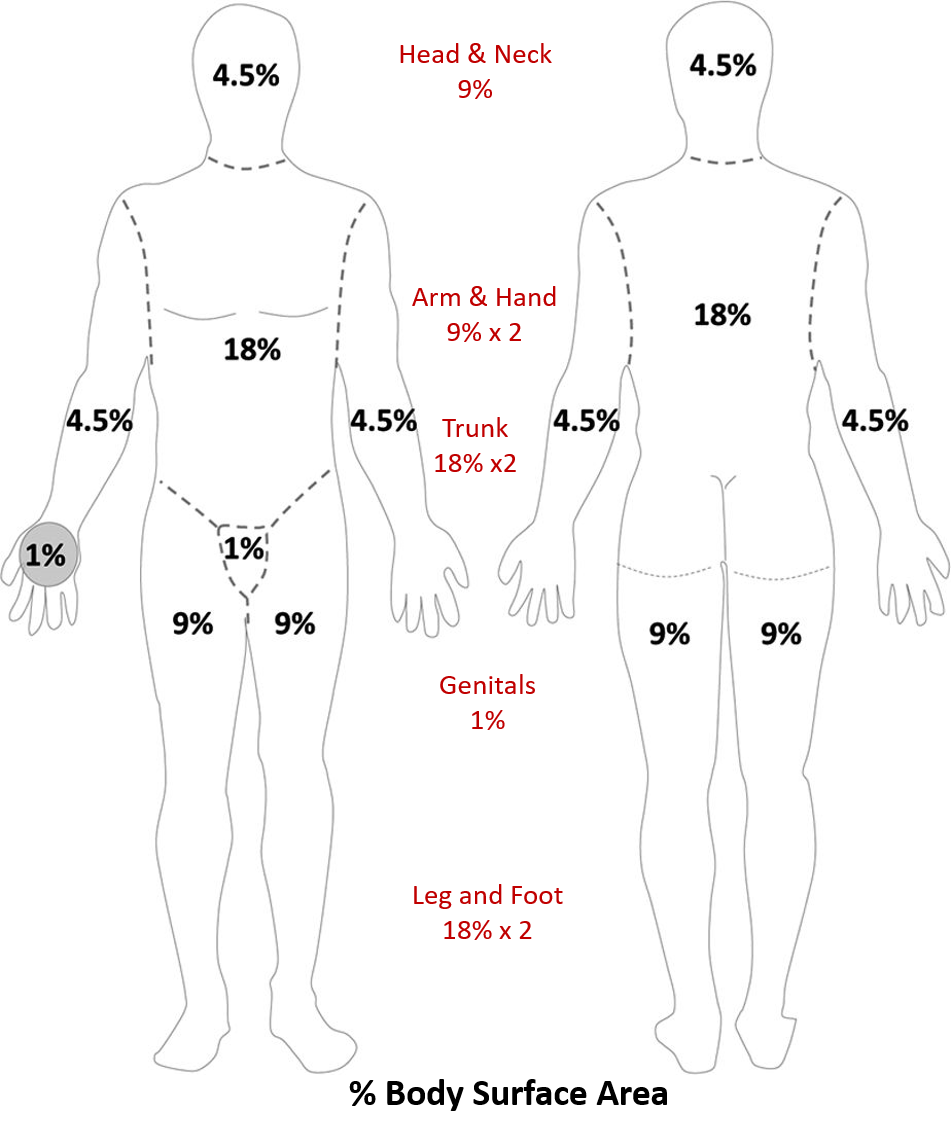
Percentage of Total Body Surface Area of the Burn – This is calculated by the ‘rule of nine’ and is of significance in second and third-degree burns. The weight and % of total body surface area (TBSA) involved help to determine the fluid loss and the amount to be replaced intravenously.
The following cases of burns should receive immediate hospital care:
- Second-degree burns >10% TBSA in children and elderly, and >20% TBSA in 11-50 years; burns involving face, hands, feet, genitals or important movable joints; and in those with significant comorbidities.
- Third-degree burns >5% in any age group.
- Electrical, lightning strike, and chemical/acid injury burns.
- Inhalation of soot, and foreign particles during fire and burn.
- Associated physical injuries like fracture, penetrating/open/bleeding wounds, etc.
Also read:
Bruise, Hematoma, Sprain-Strains, and Fracture – Managing Acute Injuries
For any query, additional information or to discuss any case, write to info@drvarsha.com, and be assured of a response soon.
References: