COPD (Chronic Obstructive Pulmonary Disease) is one of the most common conditions affecting our lower airway (respiratory tract).
How and why does COPD occur?
COPD occurs due to an inflammatory response of the lower airway (chronic bronchitis -CB) to long-term exposure to irritant substances like smoke, tobacco, industrial/factory chemicals, or environmental pollutants over a period of time. The inflammation causes narrowing of the bronchi (bronchoconstriction), which leads to difficulty in breathing and cough. COPD starts in late adulthood and is seen more in elderly people. There is commonly a history of smoking, or occupational or environmental exposure to irritants.
What are the Symptoms?
In COPD, the hallmark is a productive (wet) cough with the presence of large amounts of phlegm, which the patient needs to constantly bring out. COPD, cough with increased phlegm on waking up in the morning is characteristic, with symptoms persisting throughout the day. There is a significant impact on day-to-day exertional and work capacity, quality of life and fatigue.
COPD is a progressive condition with the bronchi getting irreversibly narrower, and symptoms worsening over time. Finally, the progressive inflammatory damage in COPD involves the air sacs in the lungs, where gaseous exchange happens (a condition called emphysema), reducing the oxygen delivery by the blood to different organs.
As COPD progresses, it can lead to serious complications and increased stress on the heart, resulting in gradual right-sided heart failure. The risk of developing respiratory infections like pneumonia and resulting complications or mortality is far higher in COPD patients.
How is COPD Diagnosed?
COPD is diagnosed mainly by history and symptoms – progressive, persistent shortness of breath (especially on exertion), chronic cough, and chronic sputum production, with a history of tobacco smoking (including pipes/cigars), occupational exposure to dusts/fumes, or indoor air pollution from biomass cooking/heating.
Chest X-rays or CT scans are used to look for signs of emphysema.
Alpha-1 antitrypsin (AAT) deficiency screening is recommended if COPD presents in patients under 45 or with a strong family history. AAT is a protein produced by the liver to protect the lungs, and its deficiency is a genetic condition causing premature or severe COPD, often called “genetic COPD,” that leads to emphysema (lower lobes) as early as age 30–40, especially in smokers
The treating physician may perform certain tests, including blood and sputum tests, and evaluation of lung function (Pulmonary Function Tests – PFT) by spirometry to assess the flow and pressures in the airway.
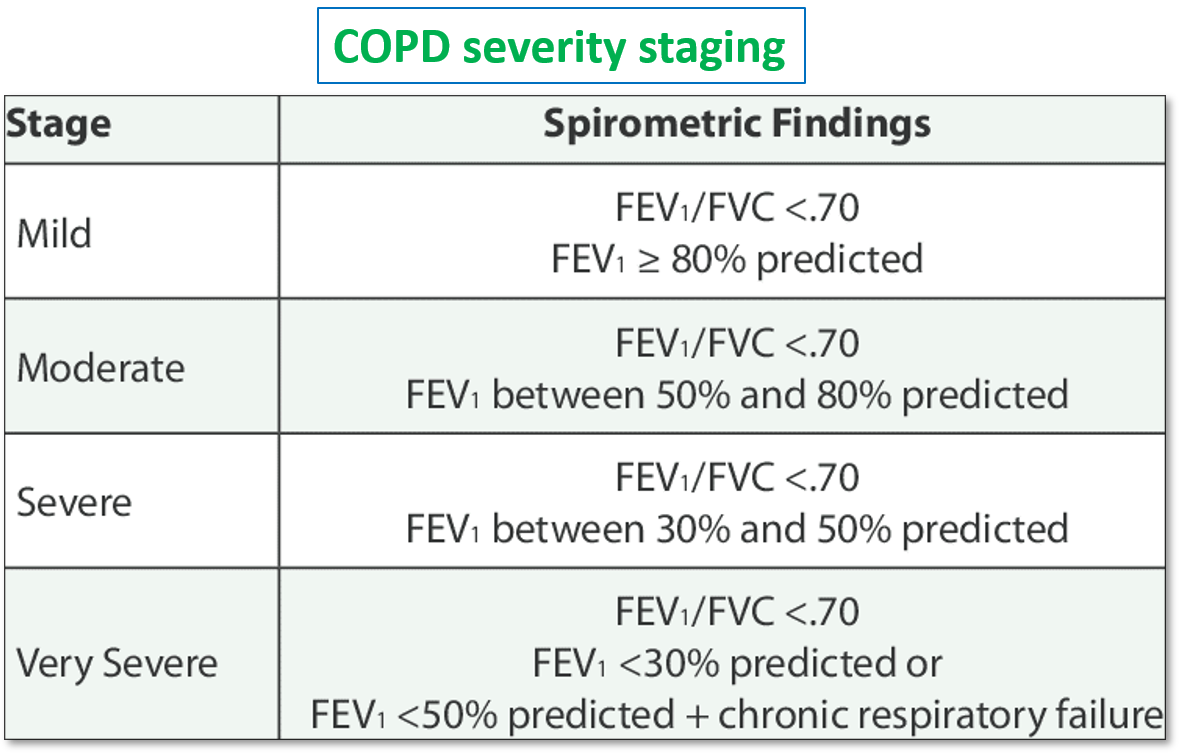
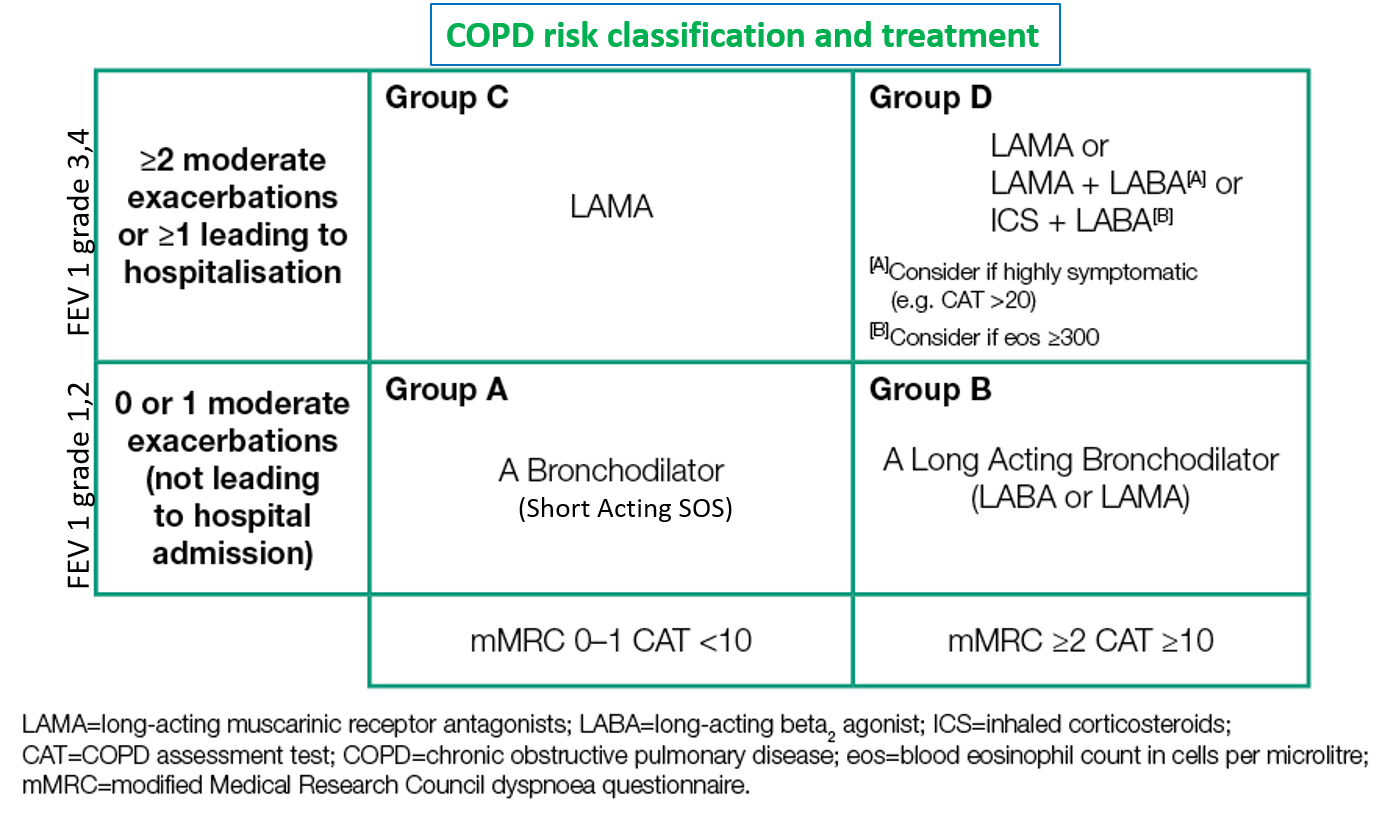
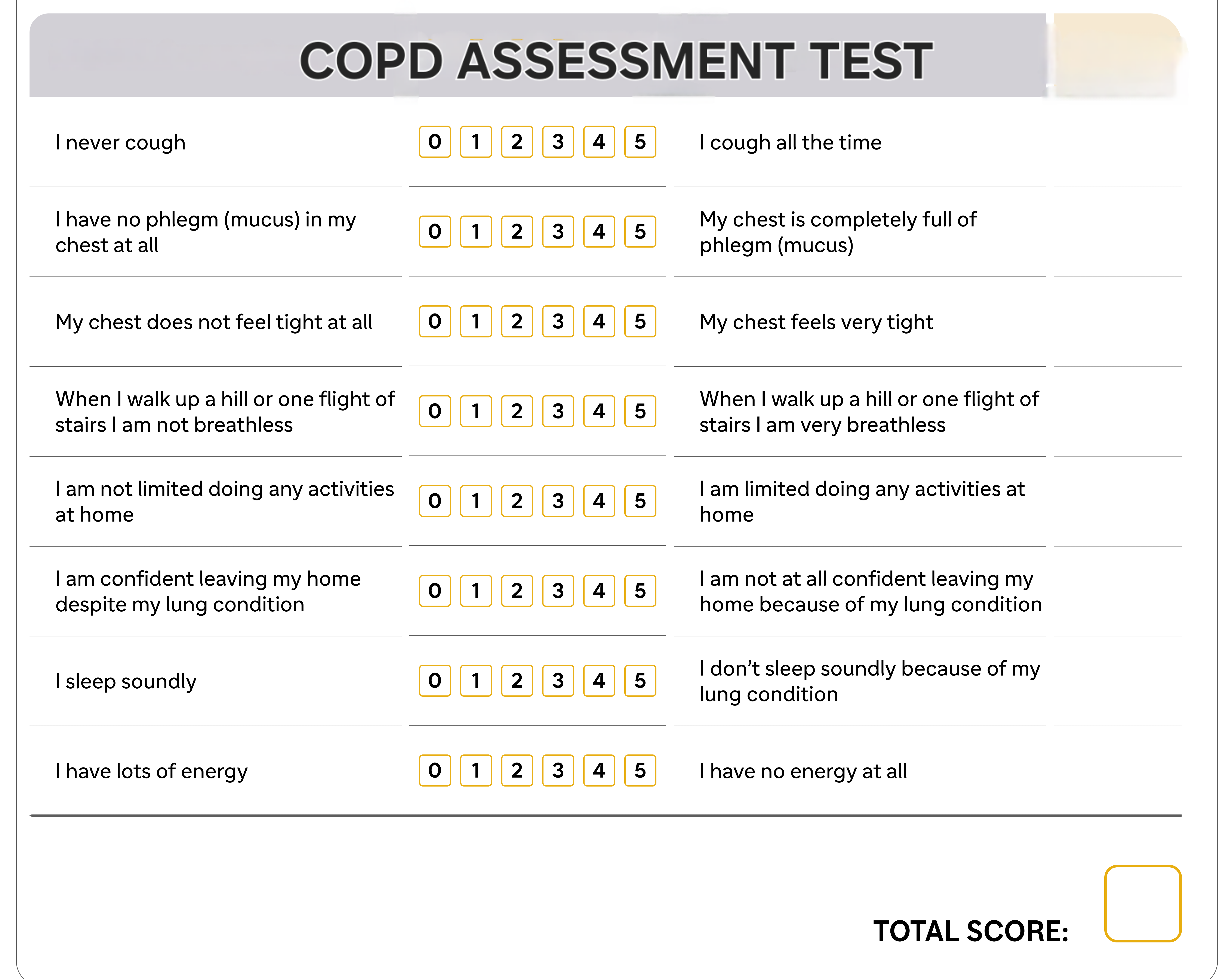
COPD is classified, and its severity is graded in accordance with the parameters on spirometry (forced expiratory volume in the first second – FEV1), symptoms or exacerbation frequency, and impact on activities of daily living (quality of life).
What Precautions should Patients with COPD take?
Irritant Avoidance: Smoking should be given up. If industrial or occupational exposure is inevitable, a change of job profile or wearing appropriate protective masks along with regular washing of the nose and mouth should be followed. Residences on the roadside or near highways or factories can also increase the frequency of exacerbation episodes in asthma and COPD.
Diet: A balanced and nutritious diet is important. Obesity or being overweight is associated with a risk of frequent exacerbations and inadequate symptom control. Such people can benefit by dropping 3-5 kg of weight through a structured diet program. Diet should be rich in fruits and vegetables, with good amounts of protein and whole grains. Overeating or very heavy meals can worsen both bloating and breathlessness.
General Health: Regular health checkups for hypertension, diabetes, BMI and heart function are important. These conditions may co-exist with COPD and worsen its course as well as increase the chances of complications.
Vaccination against influenza, pneumococcal infections, RSV, COVID-19, pertussis (Tdap), and shingles is recommended for COPD patients.
Physical activity (PA) and exercise: While a sedentary lifestyle is a risk factor for frequent exacerbation episodes as well as worse symptom control, it should be kept in mind that COPD patients may have a low capacity to exercise due to reduced oxygen availability. Therefore, a graded personalized plan should be designed for each person. Some recommended PA include:
- Aerobic exercises that use large muscle groups (like walking and yoga) instead of running or cycling.
- Strengthening exercises for the upper body, including using light weights and resistive bands, to help increase the strength of respiratory muscles.
- Yoga poses like the standing mountain pose (standing tall with arm raised as much backward to open up your chest). Standing backbends (performed very gradually) can help expand the chest to increase lung capacity.
- Effective breathing techniques practiced regularly can help enhance lung capacity, decrease breathlessness and exacerbations.
What Medicines are Available to Manage COPD?
It is important to take medications regularly according to the prescribed timing and dose. Follow-up should be regular with the treating physician for evaluation of symptom control and lung function.
Inhalers
They are most effective and easy to use, with excellent acceptance and tolerance. Inhalers can be either DPIs (Dry Powder Inhalers) or MDIs (Metered Dose Inhalers). In DPIs, a capsule containing the drug dose in powder form is inserted into the inhaler, and the powder is inhaled through a deep breath. While in MDIs, the drug is in the inhaler and is inhaled as an aerosol. Sometimes a spacer may be added to the inhaler to take in the drug more easily, especially in children. Using a nebulizer is another method of effectively giving inhalational medicines, where the medicine is inhaled as a mist through a mask.

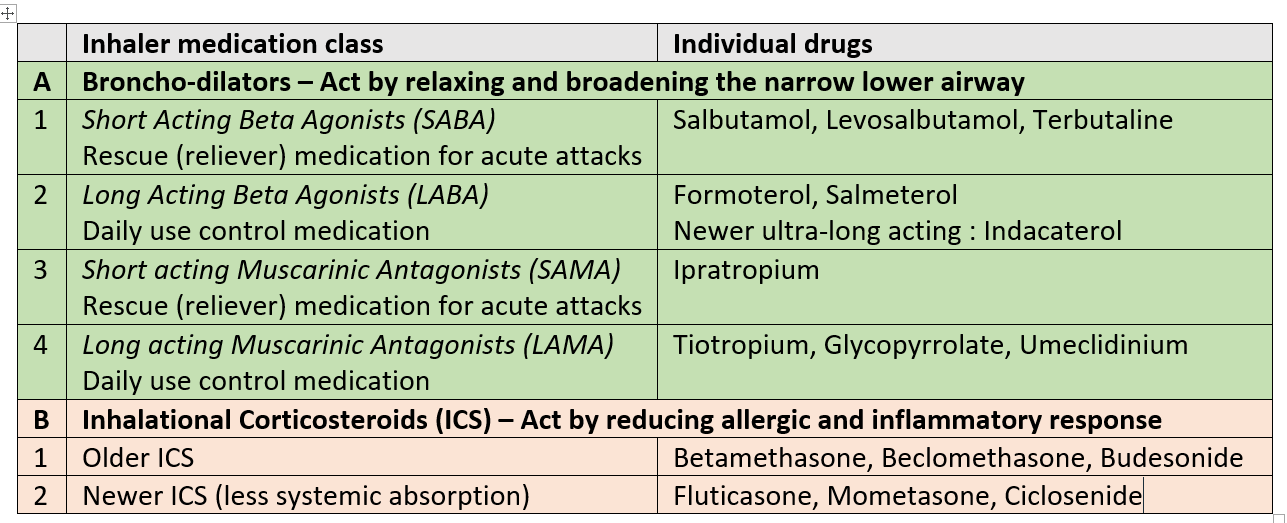
SABA and SAMA are used as reliever inhalers during breathlessness or worsening of symptoms. LABA, LAMA, and ICS are given as regular long-term anti-inflammatory controllers.
Note – Combination inhalers are commonly prescribed (SABA-SAMA, LABA-LAMA, LABA-ICS, LABA-LAMA-ICS). Other ultra-long-acting once-a-day LABAs like olodaterol and vilanterol (in combination with the ICS fluticasone) are also approved and available in some countries.
Advanced cases of COPD may require oxygen therapy.
Oral medicines
Oral medications may be prescribed as an add-on during times of exacerbations, infection or physical stress for better symptom control. These include:
- bronchodilators- etofylline-theophylline
- mucolytics- medicines to reduce and break down mucus in phlegm (acebrophylline, ambroxol, bromhexine, N-acetyl cysteine)
- expectorants- to help bring out mucus (guaiphenesin)
- specific anti-inflammatory drug approved for COPD roflumilast (PDE4 inhibitor), in poorly responsive cases.
Also read:
For any query, additional information or to discuss any case, write to info@drvarsha.com, and be assured of a response soon.
REFERENCES