WHAT ARE FIBROIDS
Fibroids are common, noncancerous muscular growths (also called leiomyomas or myomas) in the uterus, mostly during childbearing years. Uterine fibroids almost never turn into cancer and are not linked with a higher risk of other types of cancer in the uterus.
Fibroids vary in number and size from a single fibroid or more than one, sometimes too small to see, or the size of a grapefruit or larger. A fibroid that gets very big can distort the inside and the outside of the uterus, and in rare extreme cases, fill the pelvis or stomach area to give an enlarged ‘pregnant like’ appearance.
Grouping is by their location, as shown in the figure. The uterus wall consists of three distinct layers: the inner layer (endometrium) lining the uterine cavity, the thick muscular middle layer (myometrium), and the outer layer (serosa).
Intramural fibroids grow within the muscular wall (myometrium) of the uterus. Submucosal fibroids are just under the endometrium and bulge into the uterine cavity. Subserous fibroids form on the outside of the uterus.

WHY DO THEY OCCUR
The exact cause of uterine fibroids is not clear, but genetic and hormonal factors may play a role. Many fibroids contain genes that differ from those in typical uterine muscle cells. Some fibroids contain more estrogen and progesterone receptor cells than typical uterine muscle cells. Fibroids tend to shrink after menopause, and fibroids that form during pregnancy can go away after pregnancy, as hormone levels drop. Fibroids may remain stable, or grow slowly, while some may grow fast or in spurts, and shrink spontaneously. Other growth factors, such as insulin-like growth factor, may also affect fibroid growth.
Some possible risk factors seen are:
- Race. People of African race have a higher incidence of fibroids, developing at younger ages with a greater likeliness for more or larger fibroids, with worse symptoms.
- Family history. If present in mother or sister
- Menstrual factors. Starting period before the age of 10
- Metabolic factors: Obesity; Low Vitamin D; Diet higher in red meat and lower in green vegetables, fruits, and dairy; and Alcoholism.
WHAT ARE THE SYMPTOMS
Fibroids often cause no symptoms and are incidentally present for many years before a diagnosis during a routine pelvic exam or ultrasound.
Some may present with symptoms like those mentioned below, and if so, a Gynaecologist should be consulted as soon as possible:
- Heavy menstrual bleeding, longer or more frequent periods (menorrhagia and metro-menorrhagia), and bleeding/spotting in-between periods
- Painful periods (dysmenorrhea) – more painful than before
- Pelvic pressure or pain that is constant or consistent
- Pain in the stomach area or lower back, or pain during intercourse.
- Sudden, severe pain (when detached off its blood supply), seen rarely.
- Expanding feeling in the stomach region.
- Frequent urination or difficulty in urinating.
- Constipation
- Prolonged or ongoing tiredness or weakness
PROGNOSIS AND COMPLICATIONS
Uterine fibroids, though not dangerous or life-threatening, can cause pain and complications. These include anemia, due to excess blood loss during and in-between periods. Severe anemia can lead to fatigue and weakness and may require treatment including blood transfusion.
As fibroids can occur during pregnancy, they also may raise the risk of certain pregnancy complications. These include placental abruption (placenta separates from the inner wall of the uterus) and fetal growth restriction or preterm delivery before the 37th week of pregnancy.
Rarely, some fibroids, especially the submucosal ones, could cause infertility or pregnancy loss.
Fibroids may be associated with other conditions of the uterus like adenomyosis.
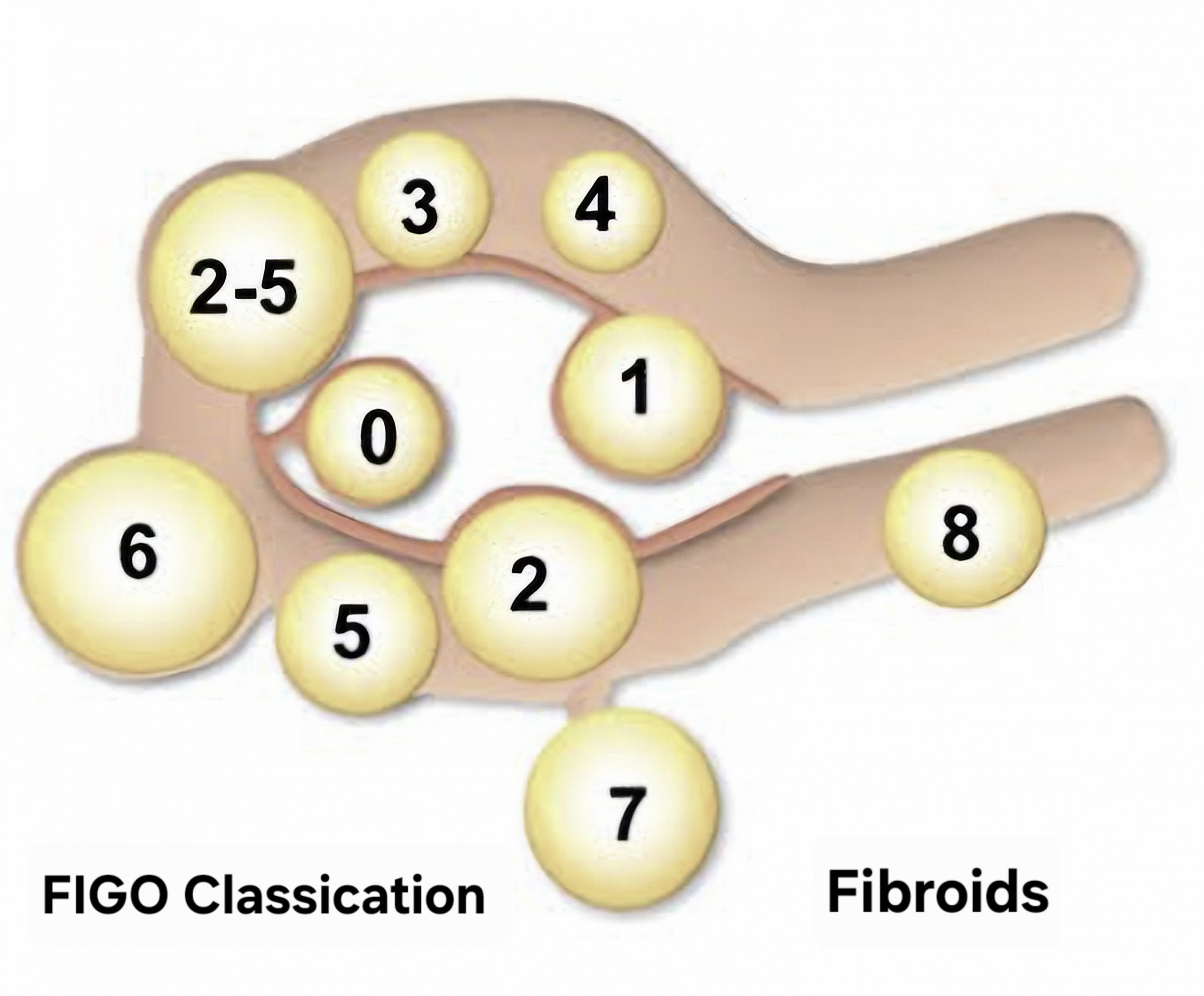
FIGO Classification of Fibroids
This classification allots a number to the fibroid according to its extent and location.
- submucosal pedunculated entirely within the uterine cavity (0)
- <50% intramural – mostly inside the cavity (1)
- >50% intramural – mostly in the wall (2)
- 100% intramural but touches the endometrium (3)
- intramural – completely within the uterine wall (4)
- subserosal – >50% intramural (5)
- subserosal <50% intramural (6)
- subserosal, pedunculated (7)
- others- cervical, parasitic, or not in the main uterine wall (8).
- hybrid or 2 numbers (2–5) describe submucosal and subserosal fibroids, with the first number indicating the endometrial relationship and the second number the serosal relationship.
This classification is used to determine if a fibroid can be removed hysteroscopically (Types 0, 1) or requires complex surgery (Types 2-6).
Hybrid fibroids 2-5, grow within the muscle wall and extend outwards, often impacting both the inner cavity and the outer contour of the uterus. These present with higher symptoms like heavy menstrual bleeding, pelvic pain, and bladder or bowel pressure, while also causing more infertility and miscarriage issues in younger women. Hybrid fibroids can be removed via hysteroscopic (if accessible), laparoscopic, or open myomectomy, and in older women by hysterectomy.
HOW ARE FIBROIDS DIAGNOSED AND TREATED
Uterine fibroids are often found by chance during a routine pelvic exam.
IMAGING
- Ultrasound (transabdominal or transvaginal) is advised in case of suggestive symptoms, or a feeling of irregular changes in the shape of the uterus on examination, suggesting the presence of fibroids.
- Hysterosonography uses saline to expand the space inside the uterus, to get better images of submucosal fibroids and the lining of the uterus.
- Hysteroscopy is done by inserting a small, lighted hysteroscope through the cervix into the uterus. Then saline is injected into the uterus to expand the uterine cavity and visualize the uterine walls and the openings of the fallopian tubes.
- Hysterosalpingography uses a dye to highlight the uterine cavity and fallopian tubes on X-ray images. This is recommended if infertility is a concern to ascertain if the fallopian tubes are open or blocked, and also view any submucosal fibroids.
- Magnetic resonance imaging (MRI). This test can show in more detail the size and location of fibroids. It can also identify different types of tumors and help determine treatment options. Most often, an MRI is used in people with a larger uterus or in those who are nearing menopause
Blood tests to check for anemia or thyroid issues are also done.
TREATMENT
Fibroids are often asymptomatic or cause mild symptoms that do not affect daily life. Since they have no malignant risk, and mostly don’t affect pregnancy either, observation and monitoring is the most appropriate management.
Medicines
Medicines for uterine fibroids target hormones that control the menstrual cycle. They treat symptoms such as heavy menstrual bleeding and pelvic pressure, and may aid in shrinking the fibroids to reduce symptoms, or facilitate easier surgery. They are of 2 types
- Gonadotropin-releasing hormone (GnRH) agonists: These suppress estrogen and progesterone synthesis, and help shrink fibroids. GnRH agonists include leuprolide, goserelin, and triptorelin. Alone these medicines can be used for a maximum of 6 months, due to troublesome hot flushes and bone loss. Symptoms return when the medicine is stopped. GnRH agonists are taken with low-dose estrogen or progestins (called add-back therapy) to ease side effects, and allow GnRH agonist treatment for up to 12 months.
- Gonadotropin-releasing hormone (GnRH) antagonists. These medicines mainly treat heavy menstrual bleeding in people with uterine fibroids, but do not shrink the fibroids. They can be used for up to 2 years. Taking them along with add-back therapy can lessen side effects such as hot flashes and bone loss. GnRH antagonists include elagolix and relugolix.
- Progestin-releasing intrauterine device (IUD): A progestin (synthetic progesterone)-releasing IUD can relieve heavy bleeding caused by fibroids. This also does not shrink fibroids or make them go away, and also prevents pregnancy.
- Low-dose birth control pills: These can help reduce menstrual bleeding, but not the fibroid size.
- Tranexamic acid (non-hormonal): This medicine reduces heavy menstrual periods and can be taken on days of heavy bleeding, but does not affect either bleeding or fibroid size.
- Nonsteroidal anti-inflammatory drugs (NSAIDs): These mainly help relieve pain and do not affect either bleeding or fibroid size
Non-invasive procedure – A non-surgical procedure called MRI-guided focused ultrasound surgery (FUS) can be considered as an outpatient way to image the precise location of fibroids by MRI and use ultrasound device focused sound waves into the fibroid to heat and destroy areas of fibroid tissue.
Minimally invasive procedures – These may have a small cut, but recovery is fast with far lesser complications than surgery. These include:
- Uterine artery embolization: Small particles called embolic agents are injected into the arteries that supply the uterus to cut off blood flow to fibroids, causing them to shrink and go away.
- Radiofrequency ablation: A laparoscope is inserted through small cuts in the stomach area or through the vagina or cervix (transvaginal or transcervical procedure) to destroy uterine fibroids and shrink its feeding blood vessels through heat from radiofrequency energy.
- Laparoscopic or robotic myomectomy: The fibroids are removed, but the uterus is left in place. This can be done laparoscopically either manually, or by a robotic system that gives the surgeon a magnified, 3D view of the uterus for better precision. Larger fibroids can be removed through smaller cuts by breaking them into pieces (called morcellation).
- Hysteroscopic myomectomy: This procedure may be an option for submucosal fibroids, removed using tools placed through the vagina and cervix into the uterus.
- Endometrial ablation: This procedure can reduce heavy menstrual flow, by inserting a device that gives off heat, microwave energy, hot water, cold temperature, or an electric current to destroy the uterine lining (endometrium). This procedure takes away the capacity of the uterus to support pregnancy, therefore, care should be taken to avoid conception, as implantation of the embryo can occur in the fallopian tube or elsewhere (ectopic pregnancy).
Conventional Surgical Procedures
This is the most definite way of preventing fibroids from recurring.
- Abdominal myomectomy. This type of surgery removes fibroids through a larger cut, especially if there is more than one fibroid, very large fibroids, or very deep fibroids. This keeps fertility and the ability to get pregnant intact, but scarring after surgery can lower the chances of future pregnancy.
- Hysterectomy. This surgery removes the uterus. It remains the only proven permanent solution for uterine fibroids, but takes away the ability to get pregnant. Hysterectomy is sometimes done with removal of ovaries as well, which brings on menopause. For all procedures except hysterectomy, fibroids can have recurrence, and these new fibroids may need treatment.
Morcellation
Morcellation is a process of breaking fibroids into smaller pieces. It can raise the risk of spreading cancer if a cancerous tumor that hadn’t been found earlier gets broken up with morcellation during a minimally invasive procedure or myomectomy. So, it is important that the surgical team looks into risk factors and cancer screening before surgery, ensures that the fibroid is broken up inside a surgical bag or the incision is expanded to remove a large fibroid without morcellation. All myomectomies carry the risk of cutting into cancer that has not been diagnosed earlier, a risk higher in women over the age of 50.
Guidelines and Recommendations
- Patient Selection and Evaluation: Preoperative cancer screening is essential. Morcellation should be avoided if imaging or biopsy raises suspicion or suggests malignancy. It is generally discouraged in women who are perimenopausal or postmenopausal.
- Tissue Containment: This recommends using containment systems (in-bag method) to limit the risk of spreading tumor tissue into the abdomen. If using a power morcellator, it should be done with a protective tube and under direct visualization
- Informed Consent: Patients must be counselled on the risks of spreading tumor tissue (leading to parasitic fibroids) or cancer.
- Surgical option: Consider abdominal hysterectomy or morcellation via a mini-laparotomy (open) or vaginal approach if the risk of cancer is deemed higher.
Also read:
Abnormal Uterine Bleeding – Understanding Causes and Manangement