India has the highest Tuberculosis (TB) burden in the world, accounting for nearly 27% of the global incidence, and approximately 2% of TB patients are estimated to be HIV positive. DR-TB (Drug-resistant-TB) constitutes around 2.5% of new cases and 13% in previously treated cases.
National TB Programs and TB Treatment Evolution in India
India has been evolving with national TB programmes, each improving upon and expanding upon the previous.
National Tuberculosis Control Programme (NTP)
The NTP that was formulated in 1962 focused on BCG vaccination and treatment at District TB centres, primarily relied on X-ray for diagnosis, and used INH (isoniazid) based and streptomycin treatment. However, NTP had low rates of detection and cure, and failed to achieve its targets.
RNTCP (Revised National Tuberculosis Control Programme)
In 1997, the RNTCP was launched, which built upon the NTP by implementing multidrug short-course anti-TB therapy (ATT) mainly as the DOTS strategy, decentralising services, and establishing sub-district supervisory units (TB Units) with dedicated supervisors, to improve case detection and treatment.
The DOTS Strategy ensured that patients took their medication under direct observation every alternate day or thrice weekly, improving treatment adherence. Sputum microscopy at Designated Microscopy Centres (DMC) was used for diagnosis. RNTCP has been credited with significantly improving case detection and treatment success rates, and is considered the largest tuberculosis control program in the world (it was expanded geographically to achieve nationwide coverage by March 2006).
RNTCP Definitions
| Case Definition | Case Type | Treatment Outcome |
| Pulmonary tuberculosis (pTB)
1. Smear+ve a) At least 2 initial sputum direct smear microscopy +ve for AFB. b) One sputum +ve with radiography consistent with active pTB c) One sputum +ve and culture +ve for Mtb. 2. Smear -ve a) Symptoms suggestive of TB, radiography consistent for active pTB, but at least 3 sputum -ve for AFB, with medical decision of treatment with full course ATT b) -ve sputum; +ve culture
|
New: Never had TB treatment or ATT beyond a month.
Relapse: Declared cured of TB by the physician, but reports back and found AFB+ve. Transferred in: Starting ATT recorded in one TB unit and then received into another TB unit. Treatment After Default: Received ATT for a month or more, but not taken ATT consecutively for 2 months or more. Failure: Smear +ve at 5 months or more post starting ATT, or who was initially sputum-ve but now found +ve during ATT. Chronic: Remains smear +ve after completing re-treatment regimen. Others: Not fitting above categories with reason specified. |
Cured: Initially smear +ve patient, completed treatment, having -ve sputum smears on two occasions, with at least one of them being after the end of ATT. |
| Treatment Completed:
a) Sputum +ve completed treatment with sputum-ve smears at the end of the initial phase, but not at the end of treatment b) Sputum -ve received full course of ATT but not smear -ve during or at the end of treatment c) Extrapulmonary TB received full course of ATT but not smear -ve during or at the end of treatment |
||
| Extrapulmonary TB (epTB)
TB in organs other than lungs (skin, pleura, lymph nodes, abdomen, genitourinary tract, bone-joints, brain/meninges). Diagnosed if a sample from any of these sites shows: a) Culture + ve b) Histological evidence c) Strong clinical evidence with medical decision of treatment with full course ATT |
Died during treatment regardless of cause.
Failure: Smear +ve at 5 months or more post starting ATT, or who was initially sputum-ve but now found +ve during ATT. Defaulted: Not taken ATT for 2 months or more consecutively after registration. Transferred out: Treatment results not known after transfer to another TB unit |
Multi Drug Resistant TB: (MDR-TB – resistant to isoniazid (H) and rifampicin (R), and RR-TB resistant to rifampicin) are major issues to be tackled. In 2022, India had a high burden of MDR/RR-TB, with an estimated 410,000 people developing the disease, and 27% of the global MDR/RR-TB cases. The prevalence of MDR-TB is 3.9% in new cases and 13.4% in previously treated cases (overall 6.7%).
Isoniazid-resistant TB (Hr-TB) refers to Mycobacterium tuberculosis strains in which resistance to isoniazid and susceptibility to rifampicin has been confirmed in vitro (KatG is a catalase-peroxidase enzyme in Mycobacterium tuberculosis that plays a crucial role in activating isoniazid and is a major cause of resistance when mutated, while InhA mutation, particularly in the promoter region, is associated with low-level resistance to isoniazid and can also confer resistance to ethionamide, a structural analog of isoniazid).
National TB Elimination Program (NTEP)
The NTEP was launched in 2020 by renaming RNTCP with the endeavour to emphasize the aim of the Government of India to eliminate TB in India by 2025, five years ahead of the global targets of 2030. The Sustainable Development Goals (SDG) targets for TB (baseline 2015) are 80% reduction in incidence, 90% reduction in mortality, and zero TB patients and their households facing catastrophic costs as a result of TB disease.
The key programme activities are implemented under 4 strategic pillars – “Detect – Treat – Prevent – Build” (DTPB). India is progressing against the SDG goals at a far greater pace than the global average, with a decline in TB incidence by 16% and in TB deaths by 18% from 2015 to 2022.
NIKSHAY is the web-enabled patient management system for TB under NTEP. It is the only public health information and communication technology system globally catering to all key stakeholders: beneficiaries, staff, and policy makers at a massive scale, managing >25% of the world’s TB burden. It supports the full digitization of the cascade of care, and is used by every healthcare worker across the country for activities spanning case management, diagnostics, adherence, direct benefit payments (social security payments), treatment outcomes, test results, and follow-up.
The NTEP has included newer MDR drugs, such as Bedaquiline (BDQ) and Delamanid (DLM), into the DOTS-Plus regimen. It has also decreased the use of injectables. Regimens with a BDQ and DLM combination have shown good culture conversion with no additive or synergistic QTc-prolongation after 6 months of treatment. The WHO has regrouped anti-TB drugs and recommended including drugs from both groups A and B to have at least 4 effective medicines in a regimen. The introduction of the DOTS-Plus treatment helped culture conversion in 63.04% of treatment failure cases but greatly increased adverse effects.10
Grouping of Medicines Recommended for Use in Longer Multi-Drug-Resistant TB regimens
| Group | Steps | Medicine | Acronym |
| A | Include all 3 medicines | Levofloxacin or Moxifloxacin
Bedaquiline Linezolid |
Lfx/Mfx
Bdq Lzd |
| B | Add 1 or both medicines | Clofazimine
Cycloserine or Terizidone |
Cfz
Cs/Trd |
| C | Add to complete the ATT regimen, and when medicines from A-B groups cannot be used | Ethambutol
Delamanid or Pretomanid Pyrazinamide Imipenem-Cilastatin or Meropenem Amikacin or Streptomycin Ethionamide or Prothionamide Para Aminosalicylic Acid |
E
Dlm/Pa Z Imp-Cln/Mpm Am/S Eto/Pto PAS |
In India, the cure rate of patients with MDR-TB with additional resistance to fluoroquinolones (MDR-TBFQ+) or second-line injectable (MDR-TBSLI+) is suboptimal and is called Pre-XDR TB. Combining 2 new drugs with 2 repurposed drugs—bedaquiline, delamanid, linezolid, and clofazimine for 24–36 weeks in adults with pulmonary MDR-TBFQ+ and/or MDR-TBSLI+, has a more favorable outcome (defined as 2 consecutive negative cultures taken 4 weeks apart).
The stress now is on Universal Drug Sensitivity Testing (DST) or liquid culture DST (LC-DST) in Culture and Drug Susceptibility Testing laboratories (C&DST) to treat each individual patient as per their requirement.
CBNAAT/GeneXpert (Cartridge-Based Nucleic Acid Amplification Test), FLLPA, and SLLPA (First and Second-line Line Probe Assay) are the pillars in the current TB strategy.
For MDR-TB, the focus is on a shorter oral regimen (BpaLM- 6-month, all-oral treatment for drug-resistant tuberculosis consisting of bedaquiline, pretomanid, linezolid, and moxifloxacin). In case of issues with one of bedaquiline or delamanid/pretomanid, a longer oral regimen may be required. For Pre-XDR, with quinolone resistance, BpaL may have to be used. Treatment of each patient needs to be individualized to achieve greater success.
NTEP Treatment Algorithm for MDR/RR-TB
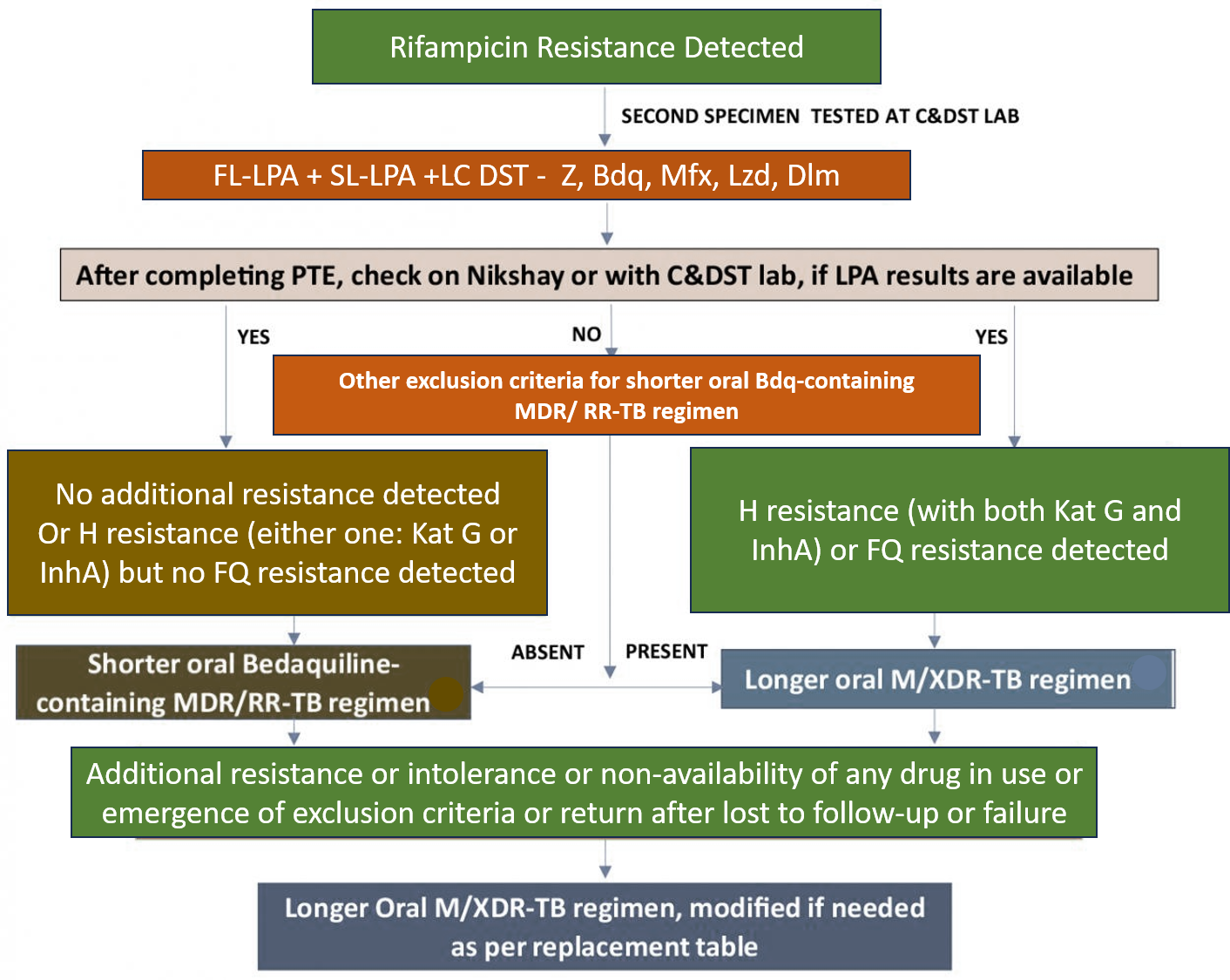
H and R Resistance is per mutation pattern, or inferred. Discordance in RR results between Nucleic Acid Amplification Tests (NAAT) & First-line Line Probe Assay (FL-LPA) to be resolved with a repeat NAAT at the Culture and Drug Susceptibility Testing (C&DST) lab, and microbiologists will provide the final decision. Use other exclusion criteria to decide the regimen if FL-LPA is done on culture isolates for patients with smear-negative specimens. Use Sl-LPA to assess Lfx, Mfx, and Am resistance. Start treatment based on Line Probe Assay (LPA) results and modify based on Liquid Culture (LC) and DST results later.
Other exclusion criteria for shorter oral Bdq-containing MDR/ RR-TB regimen include: exposure for > 1 month to Bdq, Lfx, Eto, or Cfz, if the result for DST (Bdq, FQ, Inh A mutation, Cfz & Z) is not available; Intolerance to any drug or risk of toxicity from a drug in the shorter oral Bdq-containing MDR/ RR-TB regimen (e.g., drug-drug interactions); Extensive TB disease with presence of bilateral cavitary disease or extensive parenchymal damage on chest radiography. Severe Extrapulmonary TB with presence of miliary TB or TB meningitis or CNS-TB; Pregnant and lactating women (with conditional exceptions); Children below 5 years.
NTEP moves for a shorter oral Bdq-containing MDR/ RR-TB regimen. Patients who were on a longer oral M/ XDR-TB regimen based on the history of exposure for >1 month and in whom resistance is not detected to Isoniazid (H) or FQ may be switched to shorter oral Bedaquiline containing MDR/ RR-TB regimen based on the FL and Second-line LPA (SL-LPA) results if the duration of longer oral M/ XDR-TB regimen drugs consumed is <1 month.
India has continually evolved with improved national TB programmes improving diagnosis, and incorporating more compliant treatment regimens as well as drugs for MDR-TB. It is important that private practitioners also blend into such programmes, improving access and awareness across patients of all strata. Training and raising awareness and knowledge for the same may be achieved through digital means and online education modules. National TB programmes are the most important route to achieving a TB-free India in the future.
Dr Desh Deepak is serving as Consultant Pulmonologist, at Ram Manohar Lohia Hospital, New Delhi, and has done extensive work in the field of Tuberculosis.
NTEP-Treatment algorithm for MDR/RR-TB.
Also read:
Tuberculosis (TB): Awareness, Diagnosis, Treatment, and Prevention
Interstitial Lung Disease (ILD) – Types, Risks, and Health Measures