
Whenever a person is seen to have hand tremors, the thought of Parkinson’s disease first comes to us. Often these tremors start making one withdraw socially. But not all hand tremors are due to Parkinson’s disease.
PARKINSON’S DISEASE
What is it, why does it happen and how does it present itself……
Parkinson’s disease is a result of degeneration (deterioration or slow damaging of the nervous system) and a decrease in a chemical called dopamine. It is usually seen after the age of 50 years but there are some young-onset variants. Early symptoms like tiredness, sleeping problems, constipation, or even a loss in smell may go unnoticed, till the tremor comes on.
Apart from tremor, other symptoms of Parkinson’s include slowing down and difficulty of some movements like swinging your arms, getting out of bed, taking long walking strides, and turning around which may result in moving with slow small steps, and episodes of losing balance. Also, the characteristic is the reduction in facial expressions and blinking.
Gradually mental faculties deteriorate like memory, grasping power, and reasoning, leading to confusion and forgetfulness. There may be accompanying anxiety-depression. A change in handwriting (becomes small and cramped) is characteristic with disease progression.
Advanced cases may show physical problems like drooling, difficulty in swallowing and speaking, sweating, difficulty in passing stool/urine, or inability to have an erection. As muscle weakness and stiffness slowly set in all over the body, one may be unable to stand, have pain and require assistance in moving and in many daily activities.
The classic Parkinson’s tremor, if some of the above symptoms co-present themselves, the diagnosis is pretty obvious, and usually, medicines that increase the neurochemical –dopamine and its action are administered as treatment. However, if only a tremor is seen without the other mentioned symptoms, sometimes it may be hard to be sure of the cause.
The Parkinson’s Tremor…..
Tremor is a sign in almost 80% of Parkinson’s cases and has some features which set it apart-
- Usually starts on one side and then may go on to the other side.
- Though the hand is the most common, well known and visible tremor site, Parkinson tremors can also occur in legs, feet, jaw, chin, mouth, or tongue
- Tremors of the head and voice are rare.
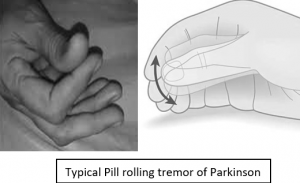
- Parkinson’s tremor has rolling typicality where the thumb rolls something on the other fingers.
- A typical Parkinson’s tremor occurs at rest (when not doing any activity).
- The tremor disappears with movement and comes back on holding something for a long time like a spoon etc.
- Apart from having social repercussions, the tremor itself usually does not interfere with daily activities.
Management of Parkinson’s Disease
Parkinson’s disease can’t be cured, but can be controlled with medications and lifestyle measures like controlled and guided physical exercise therapy to improve balance and coordination, a nutritious diet, psychological counseling, and speech therapy.
Medicines include drugs that increase dopamine levels and action. The first line and most effective drug is levodopa-carbidopa (oral combination drug Syndopa). With time and disease progression, the drug’s effect may decrease, and an increase in drug doses may produce involuntary movements called dyskinesia, thereby necessitating dose reduction and modification. Recently, an inhaled form of this drug has been made available, which can reduce some of the side effects seen with the oral pills. Duodopa is a gel form of levodopa-carbidopa for continuous intestinal administration with a portable pump directly into the duodenum or upper jejunum by a permanent tube via a procedure called percutaneous endoscopic gastrostomy.
In more advanced cases, this drug can also be given as a gel infusion through a feeding tube. A medicine called foslevodopa-foscarbidopa (also called Produodopa) has been approved to treat people with Parkinson’s who experience movement-related symptoms. Produodopa is given over 24 hours by a small pump that delivers a continuous dose of the medication from a syringe. This steady delivery helps maintain consistent dopamine levels, reducing the fluctuations in symptoms that patients often experience with other treatments.
A drug called amantadine is sometimes given to provide quick relief of symptoms in the early stages, or with levodopa-carbidopa therapy during the later stages of Parkinson’s disease to reduce dyskinesia. Anticholinergic medications (like benztropine, trihexyphenidyl) are given mainly to reduce Parkinson’s tremors.
Other drugs include dopamine mimics (agonists) like pramipexole and ropinirole (oral), rotigotine (given as a patch), and apomorphine (short-acting injection or sublingual films). Sometimes a class of drugs called MAO-B inhibitors (selegiline, rasagiline) is prescribed. These two groups of drugs are not as effective as carbidopa-levodopa, and can have psychotic side effects. They are only used as reserve medicines for the waning effects of carbidopa-levodopa. Another class of reserve drugs are the COMT inhibitors (entacapone, tolcapone) that are to be used only along with levodopa-carbidopa when its effect is wearing off. However, these drugs can worsen dyskinesias.
In advanced and non-responsive cases, a procedure called deep brain stimulation (DBS) is performed and has been seen to be effective in sustained relief.
NON-PARKINSON’S TREMORS
Even normally, tremors may be seen in the following situations:
- after exercise or sports
- stress, fear, anxiety
- exposure to cold,
- injury, lifting heavy things
- fever or infections
- on taking certain medicines
- alcohol intake or withdrawal, or too much caffeine.
These are usually temporary and should be ruled out as the cause of tremor, by observation of daily lifestyle. Some of these factors can also bring on a benign essential tremor.
Benign Essential Tremor: How is it different from Parkinson’s Disease
Another cause of tremor that is more common than Parkinson’s, often runs in families, and is also seen usually past the age of 50, is called benign essential tremor. The word ‘essential’ here relates to no cause, no other symptoms, or no other associated neurological problem being seen to exist with the tremor. ‘Benign’ means not harmful or life-threatening. The characteristics of this tremor are:
- Usually affects both sides together.
- The hands are the most commonly affected areas, but the head, neck, tongue, voice (quivering of voice), face (twitching), forearms, and even the trunk can show tremors.
- Tremors of the legs or feet are rare.
- Tremors are rapid, rather like a hand shiver, and not like the typical rolling tremor of Parkinson’s.
- Unlike the Parkinson’s tremor (seen at rest), the essential tremor is more of an action tremor and comes on usually when doing an activity like writing (handwriting can get distorted and bigger), tying or picking up something, and may very rarely occur at rest.
- Tremors may be brought on by emotional stress, fatigue, hunger, drastic temperatures, caffeinated drinks, and smoking.
Usually, essential tremor doesn’t need treatment. If it starts to interfere with daily activities, some medicines like tranquilizers or those that reduce the activity of adrenaline may be prescribed along with some physical and lifestyle advice. There are people who develop an essential tremor, but later also go on to develop Parkinson’s disease. So, it’s not as if the two are directly related but can in some cases occur in the same person.
Other Health Conditions that cause Tremors
Multiple Sclerosis (MS) is a condition in which the protective sheath covering the nerves is lost, therefore, the nerves get inflamed and damaged. The tremor in MS can occur at rest, with activity, and even while lying down. MS has a younger age of onset compared to Parkinson’s, though some of the symptoms may be similar between the two. The differentiating features are the presence in MS of extreme fatigue, difficulty in walking, pain and touch-temperature sensitivity, dizziness, vision problems, and electric shock sensations on neck movements. The slowness of movement, stiffness, loss of facial expression, and the small crawling handwriting are typical of Parkinson’s disease, not MS.
Sometimes hyperactivity of the thyroid gland can produce a fine tremor along with other symptoms like weight loss, palpitations, nervousness, inability to sleep, irritability, tiredness, heat intolerance and bulging out eyes. The gland itself may be enlarged or swollen in the neck.
Tremors may also be seen in chronic kidney disease or liver failure, sudden drop in sugar especially in people with diabetes, or after brain injury or stroke. So, running a few lab tests can help in eliminating other underlying medical problems, and landing more precisely on the diagnosis when in doubt.
Also read:
Hyperkinetic Movement Disorders – Understanding 5 Types of Dyskinesia
Dementia and Alzheimer’s Disease – Awareness, Understanding and Solutions
For any query, additional information or to discuss any case, write to info@drvarsha.com, and be assured of a response soon.
References:
National Institute of Ageing-NIH: Parkinson’s Disease
National Institute of Neurological Disorders and Stroke – Tremor fact sheet