Heart Valve Defects can be silent or present with symptoms that go unnoticed. So timely diagnosis and management is important.
TYPES
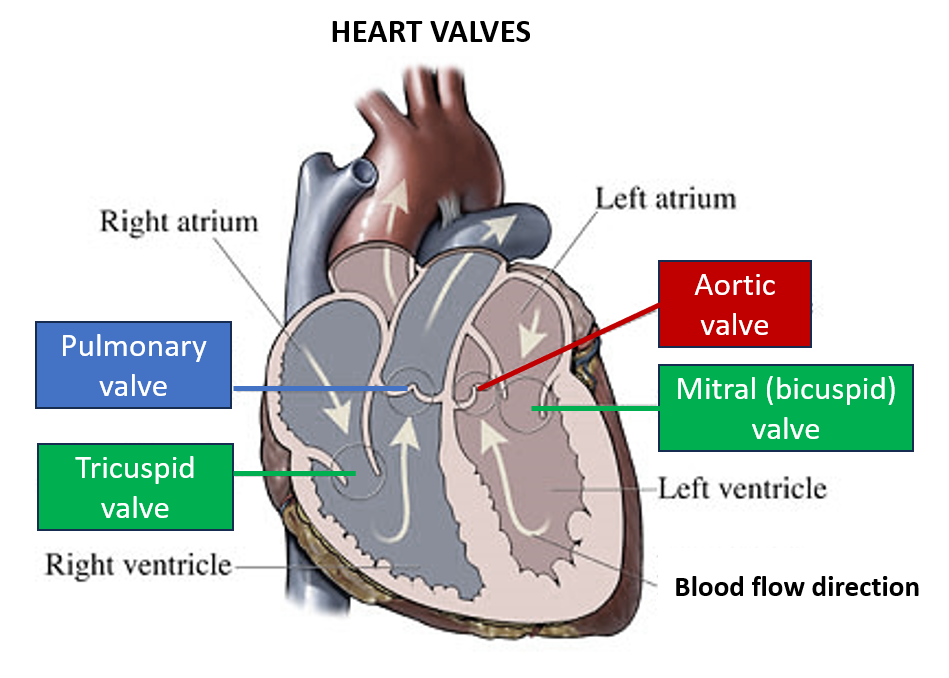
Heart valve defects can affect one or more of the four valves in the heart. Heart valves open and shut with each heartbeat to keep blood flowing in the right direction.
There are 3 types of heart valve defects:
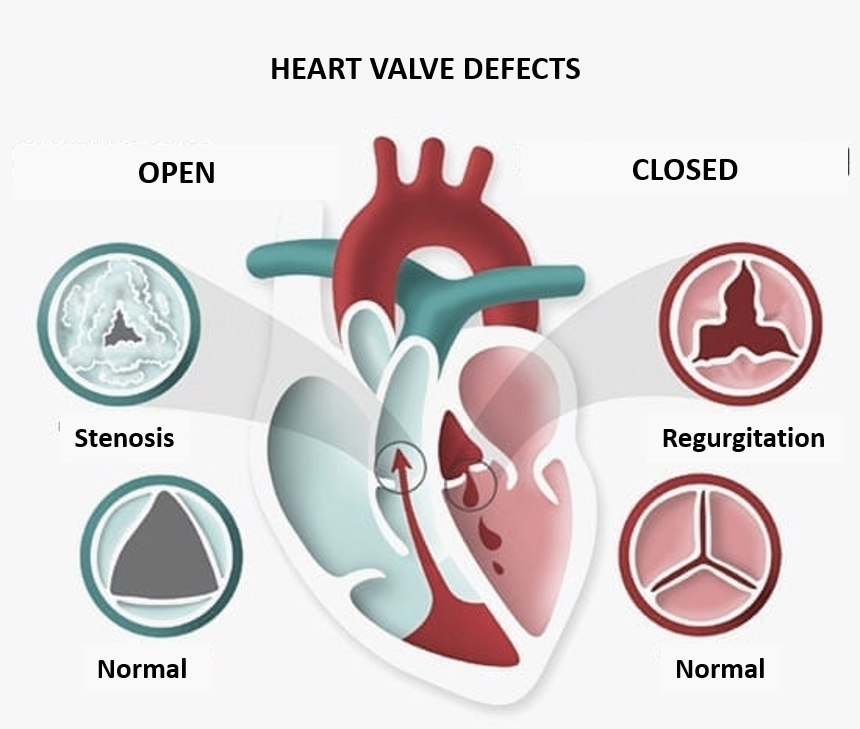
- Leaky Valves (regurgitation) – backflow of blood or prolapse of the valve
- Narrow Valves (stenosis) – decrease in blood flowing through the valve
- Abnormally developed valves without a proper opening (atresia) – lack of, or no blood flow through the valve
Valve prolapse is a condition where the flaps of the valve don’t close properly and bulge into the atrium of the heart during a heartbeat. It’s usually harmless and doesn’t require treatment unless also associated with regurgitation.
CAUSES
- Birth defects in the heart (congenital heart disease)
- Aging
- Myocardial infarction (after a heart attack)
- Infections – endocarditis, rheumatic heart disease, blood infection (bacteremia/sepsis), syphilis
- Autoimmune disorders or connective tissue disorders
- Radiation therapy to chest
- Pacemakers rubbing against valves
Other risk factors:
- Diabetes
- High blood pressure
- Obesity
- Family history of heart valve disease
SYMPTOMS
One may not experience symptoms initially, or symptoms may develop over time. These include:
- Extreme tiredness (fatigue)
- Decrease in physical work capacity
- Fainting spells or dizziness
- Breathlessness
- Chest pain
- Feeling the heart skipping a beat, fluttering, pounding, or racing
DIAGNOSIS
Many heart valve defects are picked up as abnormal sounds or ‘murmurs’ heard during auscultation of the chest with the stethoscope to listen to the heartbeat. The type of defect can be gauged by the phase in the cardiac cycle the murmur occurs.
- Systolic: Occurs when the heart contracts to pump blood. Systolic murmurs can be further divided into ejection murmurs (aortic/pulmonary stenosis) and pan-systolic murmurs (mitral/tricuspid regurgitation).
- Diastolic: Occurs when the heart relaxes between beats to fill with blood. These murmurs can be caused by a stenosis of the mitral or tricuspid valves (mid-diastolic), or regurgitation of the aortic or pulmonary valves (early diastolic).
- Continuous: Occurs throughout the heartbeat, seen in patent ductus arteriosus (PDA) and systemic arterio-venous fistulas.
The doctor may order an Electrocardiogram (ECG) to check for irregular heartbeat or abnormal rhythms, a chest X-ray, and an Echocardiogram (2-D Echo) to image the heart valves and chambers and evaluate the pumping activity and output of the heart. Echo can also be done as an exercise stress echocardiogram or as a transesophageal echocardiogram (TEE) that involves inserting a small ultrasound transducer down the esophagus to create images of the heart’s valves and chambers. Other imaging tests may include Magnetic resonance imaging (MRI) and Computed tomography (CT scan).
Timely diagnosis is important and can help prevent complications like heart rhythm problems (arrhythmia), valve infection, high blood pressure in the lungs (pulmonary hypertension), heart attack, heart failure, or cardiac arrest.
TREATMENT
Heart valve defects often need surgical intervention for repair or replacement of the valves.
Initial conservative management may be done with lifestyle modification and medicines. Lifestyle interventions include regularly monitored physical activity and exercise, stopping smoking-tobacco, weight reduction if overweight, ensuring good sleep, and reducing stress.
Medicines help to control risk factors like high blood pressure or raised cholesterol/triglycerides, and also to maintain/improve the pumping of the heart and control symptoms (like drugs to reduce heart rate and dilate blood vessels- beta-blockers or calcium channel blockers, drugs to prevent fluid accumulation in the lung, etc.- diuretics, and drug to directly improve heart pumping – digoxin).
Surgery
Surgery is the definitive treatment that can repair or replace a malfunctioning valve. Options include:
-
- Open-heart surgery: A large incision is made in the chest to repair or replace the valve, and the heart is stopped through a heart-lung bypass machine to take over the heart’s pumping function.
- Minimally invasive surgery: A catheter is threaded through a blood vessel to the heart, and the valve is repaired or replaced through that. This procedure is also known as transcatheter valve implantation (TVI) or transcatheter aortic replacement (TVR).
There are two main types of replacement heart valves:
Mechanical valve
Made of durable materials like metal, ceramic, or plastic, these valves last the longest (20-30 years), but one would need to take blood thinners for life. This is a better option for younger people.
Biological valve
Made from animal (bovine, porcine) or human tissue (donor cadavers), these valves typically last 10 to 20 years, and one usually does not need to take blood thinners for life.
Newer valves for TVI/TVR
These have valve leaflets made of biological tissue (bovine) with a frame or coating of metals (like nickel, cobalt, or chromium). These can be placed through the catheter, and expand or balloon at the site, so do not need heart surgery. These are more expensive but may enable better longevity and safety.
When choosing a replacement valve, one must consider age, life expectancy, presence of other co-morbidities, risk factors, and co-medications, as well as the economic capacity of the patient.
Also read: