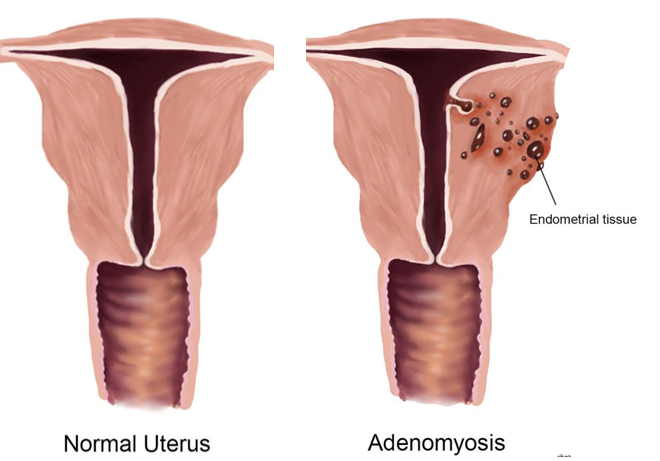
What is Adenomyosis?
Adenomyosis is a benign condition where endometrial tissue (the tissue that lines the inner cavity of the uterus) grows into the muscular wall of the uterus, causing it to thicken, enlarge, and often become painful. It is most commonly diagnosed in women who have had children (multiparous), and those in the age-group of 35–50 years are at the highest risk, with symptoms typically resolving after menopause. Adenomyosis may be associated with endometriosis or uterine fibroids.
Why does it happen?
The exact cause is unknown, but it is often linked to factors that increase estrogen levels or uterine tissue disruption or trauma, like surgeries for childbirth, miscarriage or fibroid removal.
What are the Symptoms?
It may be asymptomatic or present with symptoms like:
- Extremely heavy or long-lasting menstrual periods (menorrhagia).
- Severe, cramping pelvic pain during menstruation (dysmenorrhea).
- Chronic pelvic pain or/and
- Pain intensifies during menstruation, but may be felt throughout the cycle,
- Aching, numbness, or tingling can extend into the thighs and down the legs
- Pain during intercourse (dyspareunia).
- Feeling of pressure, fullness and bloating.
Adenomyosis can affect quality of life due to chronic pain and heavy bleeding, but symptoms generally improve or resolve after menopause when estrogen levels decline. It can cause complications in pregnancy, including preterm birth and a higher risk of miscarriage
How do you diagnose Adenomyosis?
A careful history of menstrual symptoms and pain characteristics provides the basis for suspecting adenomyosis.
Diagnostic tests include transvaginal ultrasound or MRI to identify thickened uterine walls.
A surgical or laparoscopic visualization may be needed, along with taking a biopsy to study the pathology and type of cells, and confirm the diagnosis.
While there are many grading or staging systems for adenomyosis based on clinical assessment, ultrasound, and biopsy findings, treatment decisions are primarily driven by the severity of symptoms (pain, bleeding) rather than the grade or stage. Management is individualized based on fertility desires, age, other risk factors or coexisting conditions, and lifestyle impact.
How is Adenomyosis treated?
Pain relief is the first and immediate priority for which non-steroidal anti-inflammatory drugs (NSAIDs) like ibuprofen, naproxen, etc. may be given. These may be complemented with physiotherapy and other alternative pain management techniques.
Hormonal medicines like contraceptives and GnRH-analogues, and progesterone are also given in the form of oral pills, injections, vaginal rings, intrauterine devices (IUDs) or patches
However, in those women desirous of pregnancy, fertility medicines like ovulating agents, and procedures like intrauterine insemination (IUI), and in vitro fertilization (IVF), etc. may be needed.
Surgery by key-hole (laparoscopic adenomyomectomy) is minimally invasive to remove the area of adenomyosis when confined, and to preserve the uterus. Other techniques include Uterine Artery Embolization (UAE), a procedure that cuts off blood supply to the affected area, and Endometrial Ablation that destroys the lining of the uterus.
Sometimes the entire uterus with both ovaries and tubes may be removed in older patients who have completed their family. Hysterectomy (removal of the uterus) is the only definitive cure.
Also read:
Abnormal Uterine Bleeding – Understanding Causes and Manangement
Fibroids – 5 Important Aspects of Awareness and Understanding
Endometriosis: 5 Important Points for Understanding and Awareness